

The Contribution of Surface Electromyographic Assessment for Defining the Stage of Peripheral Facial Paralysis: Flaccid or Sequelae Stage
- PMID: 30357072
- PMCID: PMC6197969
- DOI: 10.1055/s-0037-1607335
The Contribution of Surface Electromyographic Assessment for Defining the Stage of Peripheral Facial Paralysis: Flaccid or Sequelae Stage
Abstract
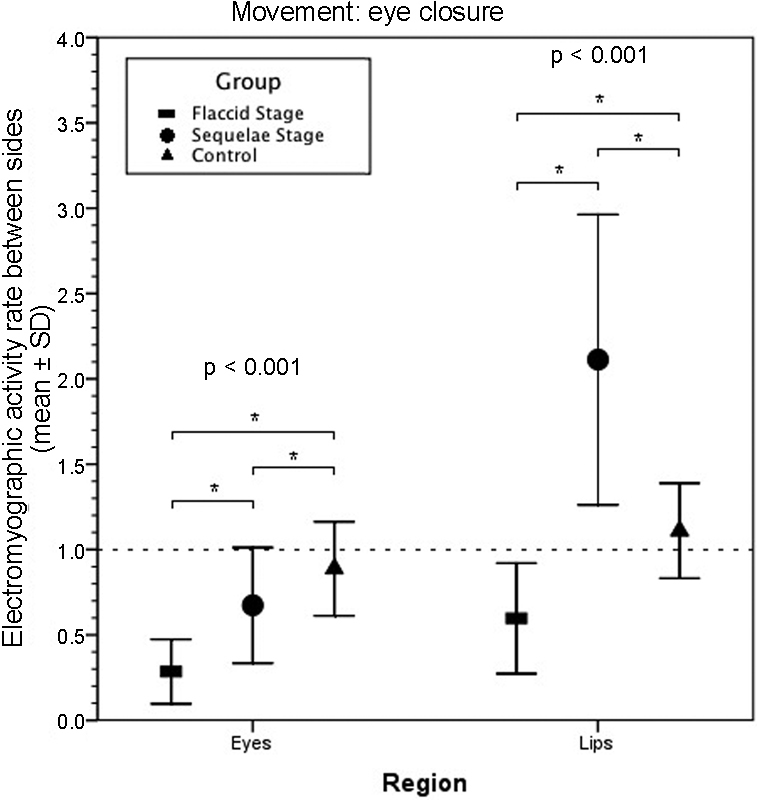
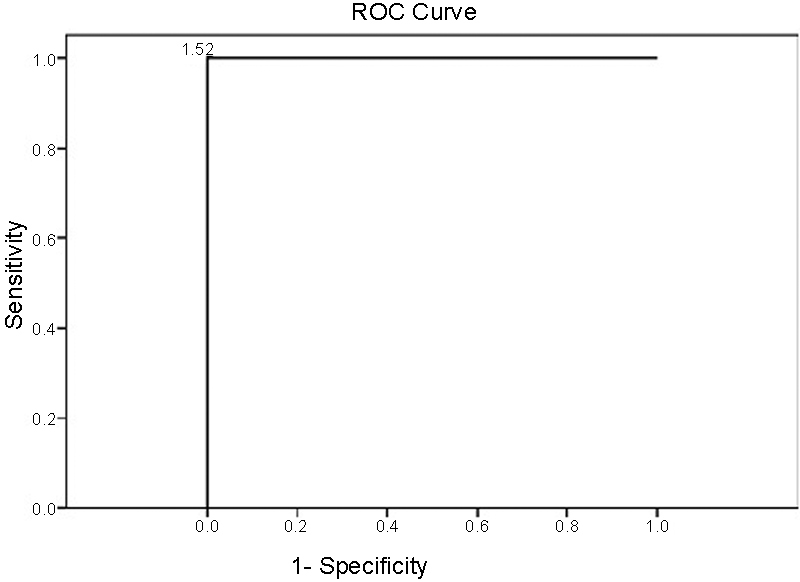
Introduction Surface electromyographic activity may not be symmetric, even in subjects with no facial paralysis history. Objective To evaluate the contribution of the index of electromyographic (IEMG) activity in the identification of the two extremes of the facial paralysis course. Methods Thirty-four subjects with unilateral peripheral facial paralysis were selected. A control group was composed of volunteers without a history of facial paralysis. The electromyographic assessment of the facial muscle was performed by placing surface electrodes during movements of the forehead, eyes and lips using MIOTEC equipment, such as the MIOTOOL (Miotec, Porto Alegre, Brazil) software. The electromyographic activity was also recorded in other channels during the primary activity to identify the presence of synkinesis. The statistical analysis was performed using the Statistical Package for Social Sciences for Macintosh (SPSS Inc, Chicago, IL, USA). The IEMG activity was obtained from the division of the electromyographic activity root mean square (RMS) values on both sides. Results There was a statistically significant difference among the groups in all the analyzed indexes. The ocular-oral synkinesis in all patients must be correctly identified (with 100% sensitivity and specificity) using an IEMG activity of 1.62 as a cutoff point. The oral-ocular synkinesis must be correctly identified (93.3% sensitivity and 95.9% specificity) using the IEMG activity of 1.79 as a cutoff point. Conclusion The IEMG activity is below the normal scores in patients in the flaccid stage, whereas patients in the sequelae stage can either show normal values or values above or below the normal scores. The IEMG activity was shown to have high sensitivity and specificity in the identification of synkinesis.
Keywords: electromyography; facial paralysis; surface.
Figures




References
-
- Bento R F. São Paulo: Edusp; 1998. Doenças do Nervo Facial; pp. 427–459.
-
- Lazarini P R, Costa H JZR, Camargo A CK. São Paulo: Lovise; 2006. Anatomo-fisiologia e fisiopatologia do Nervo Facial; pp. 25–32.
-
- Vanswearingen J. Facial rehabilitation: a neuromuscular reeducation, patient-centered approach. Facial Plast Surg. 2008;24(02):250–259. - PubMed
-
- Rosson G D, Redett R J. Facial palsy: anatomy, etiology, grading, and surgical treatment. J Reconstr Microsurg. 2008;24(06):379–389. - PubMed
-
- Sunderland S. The anatomy and physiology of nerve injury. Muscle Nerve. 1990;13(09):771–784. - PubMed
LinkOut - more resources
Full Text Sources