

Management of arterial hypertension with angiotensin receptor blockers: Current evidence and the role of olmesartan
- PMID: 30358114
- PMCID: PMC6587798
- DOI: 10.1111/1755-5922.12471
Management of arterial hypertension with angiotensin receptor blockers: Current evidence and the role of olmesartan
Abstract
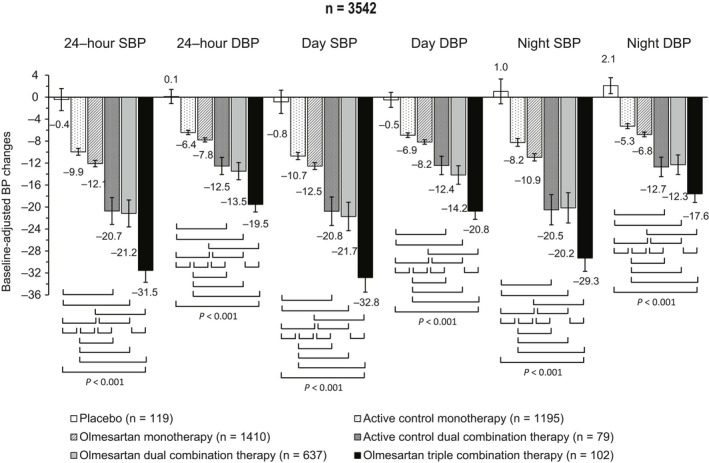
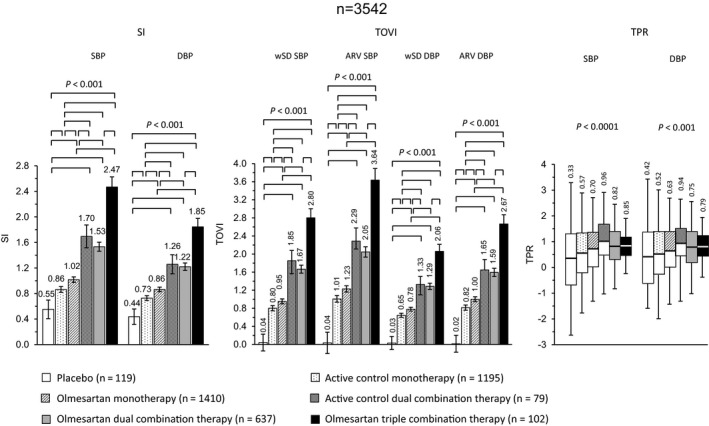
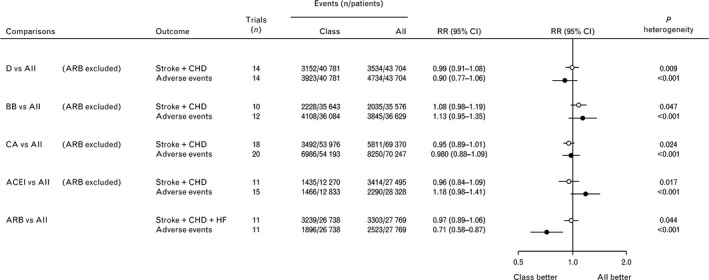
Elevated blood pressure (BP) is a major determinant of morbidity and mortality burden related to cardio-metabolic risk. Current guidelines indicate that controlling and lowering BP promotes cardiovascular (CV) risk reduction. Among antihypertensive agents, angiotensin receptor blockers (ARBs) are characterized by an efficacy profile equivalent to other antihypertensive agents and are provided with excellent tolerability and low discontinuation rates during chronic treatments. Moreover, CV outcomes are reduced by ARBs. Olmesartan is a long-lasting ARB which proved to achieve a comparable or more effective action in lowering BP when compared to other ARBs. Olmesartan, in fact, displayed a larger and more sustained antihypertensive effect over the 24 hours, with a buffering effect on short-term BP variability. These are important features which differentiate olmesartan from the other principles of the same class and that may help to control the increased CV risk in the presence of high BP variability. Olmesartan shows similar benefits as other ARBs in terms of all-cause and CV mortality, and a favorable tolerability profile. Combination of olmesartan with long-lasting calcium-channel blockers and thiazide diuretics represents a rational and effective therapy. Thus, ARBs, including olmesartan, represent one of the most effective and safe treatments for patients with arterial hypertension.
Keywords: ambulatory blood pressure; angiotensin receptor blockers; arterial hypertension; blood pressure; blood pressure variability; olmesartan.
© 2018 The Authors. Cardiovascular Therapeutics Published by John Wiley & Sons Ltd.
Conflict of interest statement
SO and MV received a grant for the preparation of the manuscript.
Figures
Similar articles
-
Triple Combination Therapies Based on Olmesartan: A Personalized Therapeutic Approach to Improve Blood Pressure Control.High Blood Press Cardiovasc Prev. 2017 Sep;24(3):255-263. doi: 10.1007/s40292-017-0217-0. Epub 2017 Jun 12. High Blood Press Cardiovasc Prev. 2017. PMID: 28608025 Review.
-
Monotherapy and Dual Combination Therapies Based on Olmesartan: A Comprehensive Strategy to Improve Blood Pressure Control.High Blood Press Cardiovasc Prev. 2017 Sep;24(3):243-253. doi: 10.1007/s40292-017-0216-1. Epub 2017 Jun 12. High Blood Press Cardiovasc Prev. 2017. PMID: 28608026 Review.
-
Olmesartan/amlodipine: a review of its use in the management of hypertension.Vasc Health Risk Manag. 2011;7:183-92. doi: 10.2147/VHRM.S16852. Epub 2011 Mar 29. Vasc Health Risk Manag. 2011. PMID: 21490944 Free PMC article. Review.
-
Olmesartan medoxomil-based antihypertensive therapy evaluated by ambulatory blood pressure monitoring: efficacy in high-risk patient subgroups.Am J Cardiovasc Drugs. 2012 Dec 1;12(6):375-89. doi: 10.1007/BF03262472. Am J Cardiovasc Drugs. 2012. PMID: 23116225 Review.
-
Rationale, design and patient baseline characteristics of OlmeSartan and calcium antagonists randomized (OSCAR) study: a study comparing the incidence of cardiovascular events between high-dose angiotensin II receptor blocker (ARB) monotherapy and combination therapy of ARB with calcium channel blocker in Japanese elderly high-risk hypertensive patients (ClinicalTrials. gov no. NCT00134160).Hypertens Res. 2009 Jul;32(7):575-80. doi: 10.1038/hr.2009.60. Epub 2009 May 15. Hypertens Res. 2009. PMID: 19444280 Clinical Trial.
Cited by
-
Herbal Medicine for Cardiovascular Diseases: Efficacy, Mechanisms, and Safety.Front Pharmacol. 2020 Apr 7;11:422. doi: 10.3389/fphar.2020.00422. eCollection 2020. Front Pharmacol. 2020. PMID: 32317975 Free PMC article. Review.
-
The protective effects of Olmesartan against interleukin-29 (IL-29)-induced type 2 collagen degradation in human chondrocytes.Bioengineered. 2022 Jan;13(1):1802-1813. doi: 10.1080/21655979.2021.1997090. Bioengineered. 2022. Retraction in: Bioengineered. 2024 Dec;15(1):2299551. doi: 10.1080/21655979.2024.2299551. PMID: 35012432 Free PMC article. Retracted.
-
Antihypertensive Indigenous Lebanese Plants: Ethnopharmacology and a Clinical Trial.Biomolecules. 2019 Jul 20;9(7):292. doi: 10.3390/biom9070292. Biomolecules. 2019. PMID: 31330767 Free PMC article. Clinical Trial.
-
Prescribing trends and patterns for antihypertensive agents in primary healthcare settings in Qatar: a retrospective observational study.J Pharm Policy Pract. 2025 Jun 18;18(1):2512183. doi: 10.1080/20523211.2025.2512183. eCollection 2025. J Pharm Policy Pract. 2025. PMID: 40547565 Free PMC article.
-
ARB-Based Combination Therapy for the Clinical Management of Hypertension and Hypertension-Related Comorbidities: A Spotlight on Their Use in COVID-19 Patients.High Blood Press Cardiovasc Prev. 2021 May;28(3):255-262. doi: 10.1007/s40292-021-00443-z. Epub 2021 Mar 12. High Blood Press Cardiovasc Prev. 2021. PMID: 33710599 Free PMC article. Review.
References
-
- GBD 2015 Mortality and Causes of Death Collaborators . Global, regional, and national life expectancy, all‐cause mortality, and cause‐specific mortality for 249 causes of death, 1980‐2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388(10053):1459‐1544. - PMC - PubMed
-
- Global Burden of Metabolic Risk Factors for Chronic Diseases Collaboration . Global Burden of Metabolic Risk Factors for Chronic Diseases Collaboration. Cardiovascular disease, chronic kidney disease, and diabetes mortality burden of cardiometabolic risk factors from 1980 to 2010: a comparative risk assessment. Lancet Diabetes Endocrinol. 2014;2(8):634‐647. - PMC - PubMed
-
- GBD 2013 Risk Factors Collaborators , Forouzanfar MH, Alexander L, Anderson HR, et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks in 188 countries, 1990‐2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;386(10010):2287‐2323. - PMC - PubMed
-
- Lewington S, Clarke R, Qizilbash N, Peto R, Collins R. Prospective Studies Collaboration. Age‐specific relevance of usual blood pressure to vascular mortality: a meta‐analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002;360(9349):1903‐1913. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
