

Predictive Modeling for Geriatric Hip Fracture Patients: Early Surgery and Delirium Have the Largest Influence on Length of Stay
- PMID: 30358636
- PMCID: PMC6411423
- DOI: 10.5435/JAAOS-D-17-00447
Predictive Modeling for Geriatric Hip Fracture Patients: Early Surgery and Delirium Have the Largest Influence on Length of Stay
Abstract
Background: Averaging length of stay (LOS) ignores patient complexity and is a poor metric for quality control in geriatric hip fracture programs. We developed a predictive model of LOS that compares patient complexity to the logistic effects of our institution's hip fracture care pathway.
Methods: A retrospective analysis was performed on patients enrolled into a hip fracture co-management pathway at an academic level I trauma center from 2014 to 2015. Patient complexity was approximated using the Charlson Comorbidity Index and ASA score. A predictive model of LOS was developed from patient-specific and system-specific variables using a multivariate linear regression analysis; it was tested against a sample of patients from 2016.
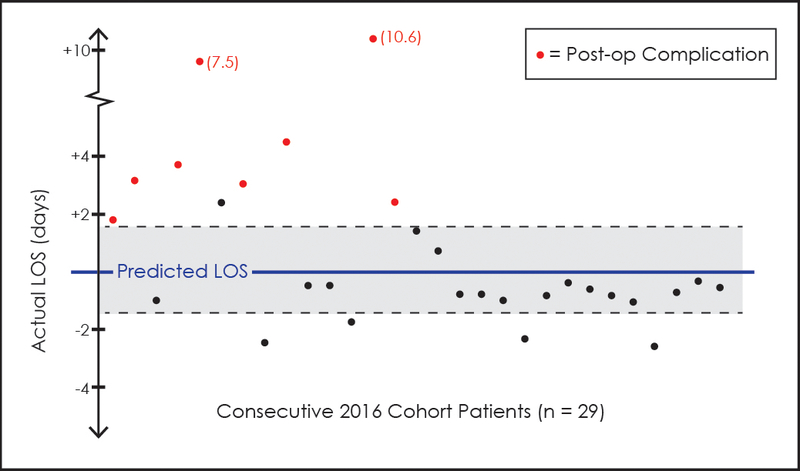
Results: LOS averaged 5.95 days. Avoidance of delirium and reduced time to surgery were found to be notable predictors of reduced LOS. The Charlson Comorbidity Index was not a strong predictor of LOS, but the ASA score was. Our predictive LOS model worked well for 63% of patients from the 2016 group; for those it did not work well for, 80% had postoperative complications.
Discussion: Predictive LOS modeling accounting for patient complexity was effective for identifying (1) reasons for outliers to the expected LOS and (2) effective measures to target for improving our hip fracture program.
Level of evidence: III.
Conflict of interest statement
Conflict of Interest: The authors declare that they have no conflict of interest.
Figures
References
-
- Braithwaite RS, Col NF, Wong JB, 2003. Estimating hip fracture morbidity, mortality and costs. J Am Geriatr Soc 51, 364–370. - PubMed
-
- Kates SL, 2016. Hip fracture programs: are they effective? Injury 47 Suppl 1, S25–27. - PubMed
-
- Lefaivre KA, Macadam SA, Davidson DJ, Gandhi R, Chan H, Broekhuyse HM, 2009. Length of stay, mortality, morbidity and delay to surgery in hip fractures. J Bone Joint Surg Br 91, 922–927. - PubMed
