

Progression of myocardial fibrosis in hypertrophic cardiomyopathy: mechanisms and clinical implications
- PMID: 30358845
- PMCID: PMC6343081
- DOI: 10.1093/ehjci/jey135
Progression of myocardial fibrosis in hypertrophic cardiomyopathy: mechanisms and clinical implications
Abstract
Aims: Myocardial fibrosis as detected by late gadolinium enhancement (LGE) on cardiac magnetic resonance (CMR) is a powerful prognostic marker in hypertrophic cardiomyopathy (HCM) and may be progressive. The precise mechanisms underlying fibrosis progression are unclear. We sought to assess the extent of LGE progression in HCM and explore potential causal mechanisms and clinical implications.
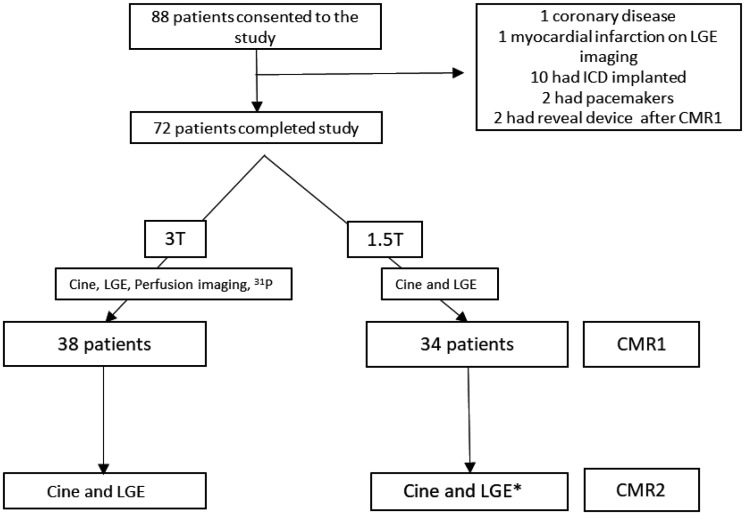
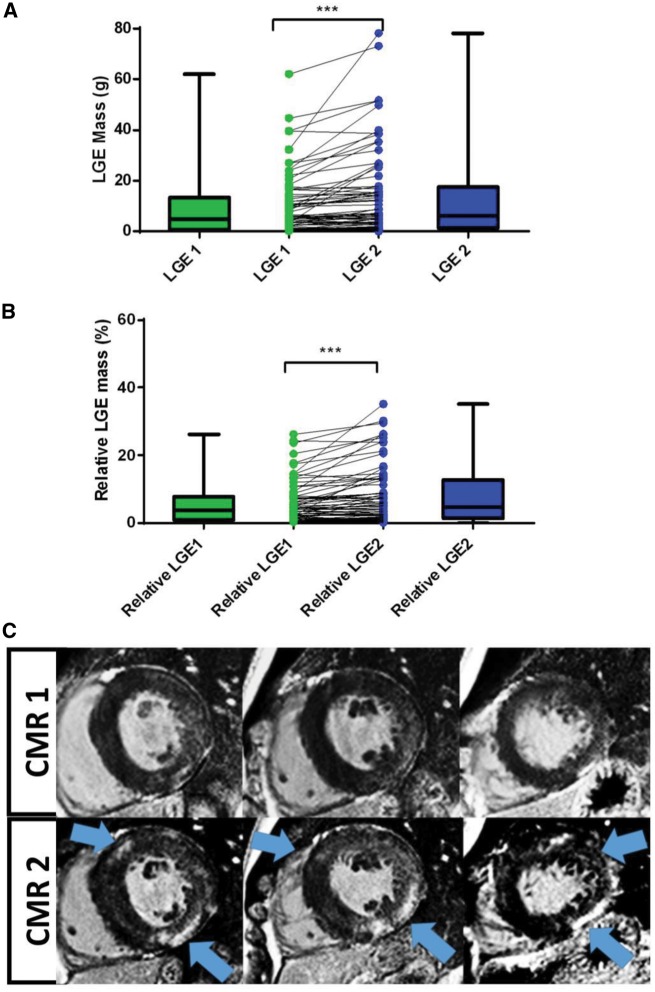
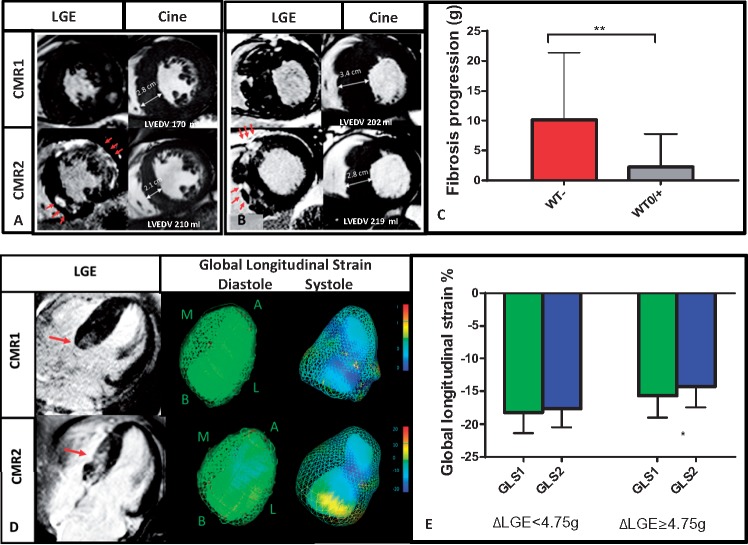
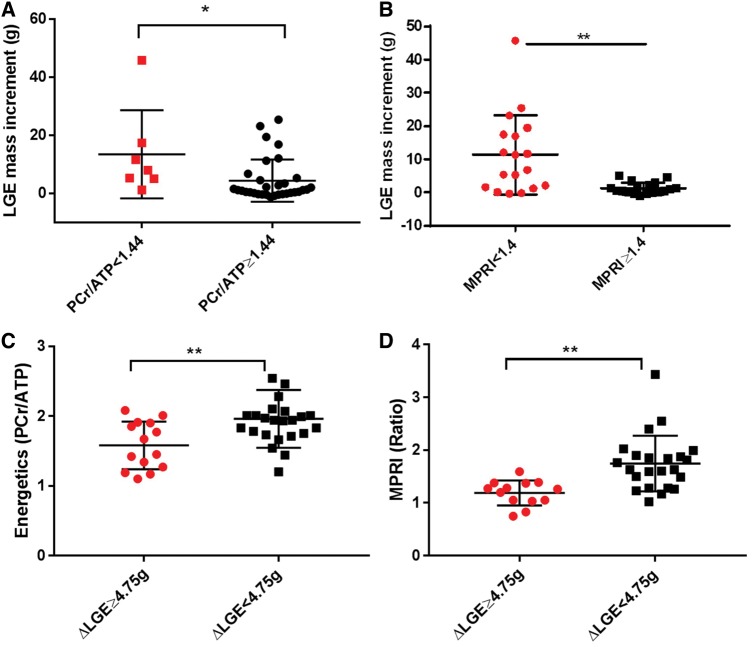
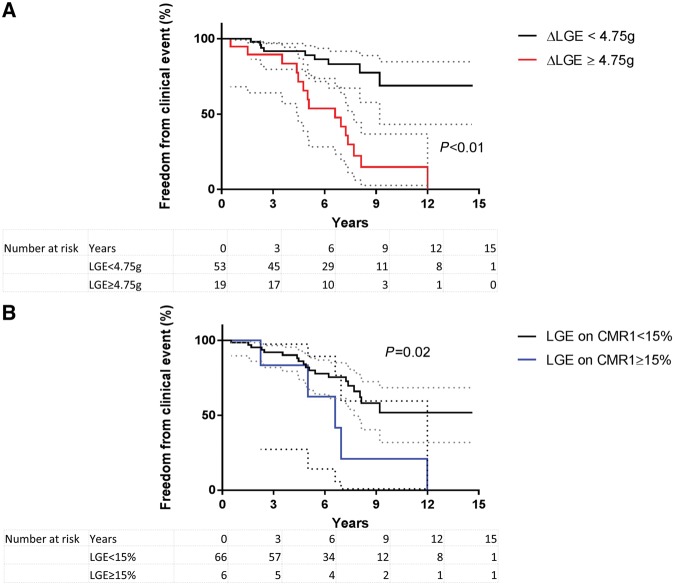
Methods and results: Seventy-two HCM patients had two CMR (CMR1-CMR2) at an interval of 5.7 ± 2.8 years with annual clinical follow-up for 6.3 ± 3.6 years from CMR1. A combined endpoint of heart failure progression, cardiac hospitalization, and new onset ventricular tachycardia was assessed. Cine and LGE imaging were performed to assess left ventricular (LV) mass, function, and fibrosis on serial CMR. Stress perfusion imaging and cardiac energetics were undertaken in 38 patients on baseline CMR (CMR1). LGE mass increased from median 4.98 g [interquartile range (IQR) 0.97-13.48 g] to 6.30 g (IQR 1.38-17.51 g) from CMR1 to CMR2. Substantial LGE progression (ΔLGE ≥ 4.75 g) occurred in 26% of patients. LGE increment was significantly higher in those with impaired myocardial perfusion reserve (<MPRI 1.40) and energetics (phosphocreatine/adenosine triphosphate <1.44) on baseline CMR (P ≤ 0.01 for both). Substantial LGE progression was associated with LV thinning, increased cavity size and reduced systolic function, and conferred a five-fold increased risk of subsequent clinical events (hazard ratio 5.04, 95% confidence interval 1.85-13.79; P = 0.002).
Conclusion: Myocardial fibrosis is progressive in some HCM patients. Impaired energetics and perfusion abnormalities are possible mechanistic drivers of the fibrotic process. Fibrosis progression is associated with adverse cardiac remodelling and predicts an increased risk of subsequent clinical events in HCM.
Figures
References
-
- Elliott PM, Poloniecki J, Dickie S, Sharma S, Monserrat L, Varnava A. et al. Sudden death in hypertrophic cardiomyopathy: identification of high risk patients. J Am Coll Cardiol 2000;36:2212–8. - PubMed
-
- Mavrogeni S, Petrou E, Kolovou G, Theodorakis G, Iliodromitis E.. Prediction of ventricular arrhythmias using cardiovascular magnetic resonance. Eur Heart J Cardiovasc Imaging 2013;14:518–25. - PubMed
-
- Shirani J, Pick R, Roberts WC, Maron BJ.. Morphology and significance of the left ventricular collagen network in young patients with hypertrophic cardiomyopathy and sudden cardiac death. J Am Coll Cardiol 2000;35:36–44. - PubMed
-
- Galati G, Leone O, Pasquale F, Olivotto I, Biagini E, Grigioni F. et al. Histological and histometric characterization of myocardial fibrosis in end-stage hypertrophic cardiomyopathy: a clinical-pathological study of 30 explanted hearts. Circ Heart Fail 2016;9:e003090. - PubMed
-
- Moon JC, Sheppard M, Reed E, Lee P, Elliott PM, Pennell DJ.. The histological basis of late gadolinium enhancement cardiovascular magnetic resonance in a patient with Anderson-Fabry disease. J Cardiovasc Magn Reson 2006;8:479–82. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
