

Development of Clinical Criteria for Functional Assessment to Predict Primary Nonfunction of High-Risk Livers Using Normothermic Machine Perfusion
- PMID: 30359490
- PMCID: PMC6659387
- DOI: 10.1002/lt.25291
Development of Clinical Criteria for Functional Assessment to Predict Primary Nonfunction of High-Risk Livers Using Normothermic Machine Perfusion
Abstract
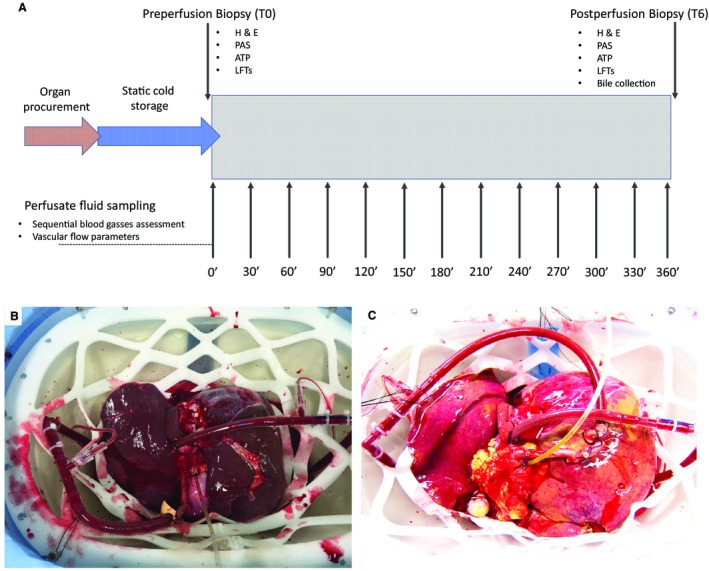
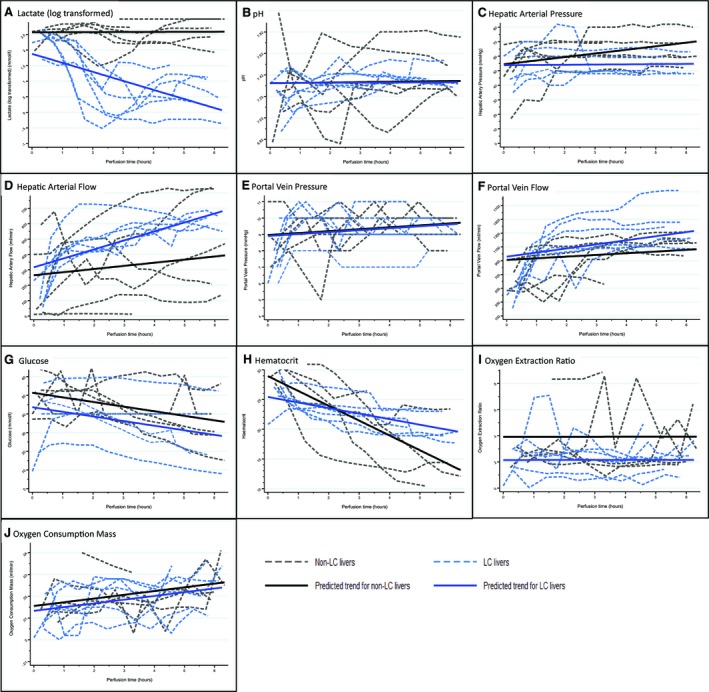
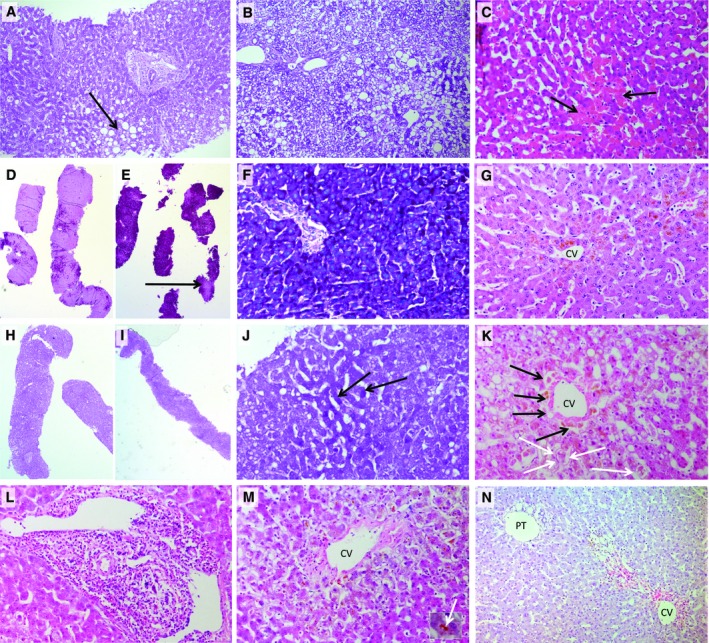
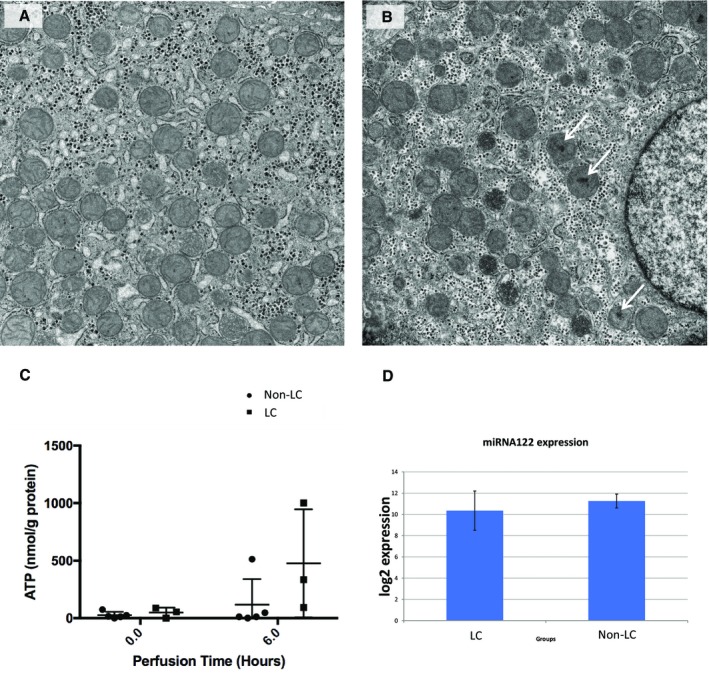
Increased use of high-risk allografts is critical to meet the demand for liver transplantation. We aimed to identify criteria predicting viability of organs, currently declined for clinical transplantation, using functional assessment during normothermic machine perfusion (NMP). Twelve discarded human livers were subjected to NMP following static cold storage. Livers were perfused with a packed red cell-based fluid at 37°C for 6 hours. Multilevel statistical models for repeated measures were employed to investigate the trend of perfusate blood gas profiles and vascular flow characteristics over time and the effect of lactate-clearing (LC) and non-lactate-clearing (non-LC) ability of the livers. The relationship of lactate clearance capability with bile production and histological and molecular findings were also examined. After 2 hours of perfusion, median lactate concentrations were 3.0 and 14.6 mmol/L in the LC and non-LC groups, respectively. LC livers produced more bile and maintained a stable perfusate pH and vascular flow >150 and 500 mL/minute through the hepatic artery and portal vein, respectively. Histology revealed discrepancies between subjectively discarded livers compared with objective findings. There were minimal morphological changes in the LC group, whereas non-LC livers often showed hepatocellular injury and reduced glycogen deposition. Adenosine triphosphate levels in the LC group increased compared with the non-LC livers. We propose composite viability criteria consisting of lactate clearance, pH maintenance, bile production, vascular flow patterns, and liver macroscopic appearance. These have been tested successfully in clinical transplantation. In conclusion, NMP allows an objective assessment of liver function that may reduce the risk and permit use of currently unused high-risk livers.
© 2018 by the American Association for the Study of Liver Diseases.
Figures
Comment in
-
Viability Criteria for Functional Assessment of Donor Livers During Normothermic Machine Perfusion.Liver Transpl. 2018 Oct;24(10):1333-1335. doi: 10.1002/lt.25330. Liver Transpl. 2018. PMID: 30193403 No abstract available.
References
-
- Williams R, Ashton K, Aspinall R, Bellis MA, Bosanquet J, Cramp ME, et al. Implementation of the Lancet Standing Commission on Liver Disease in the UK. Lancet 2015;386:2098‐2111. - PubMed
-
- National Health Service Blood and Transplant . Organ Donation and Transplantation: Activity Report 2016/17. www.odt.nhs.uk. Accessed October 13, 2017.
-
- Walker KG, Eastmond CJ, Best PV, Matthews K. Eosinophilia‐myalgia syndrome associated with prescribed L‐tryptophan. Lancet 1990;336:695‐696. - PubMed
-
- Ploeg RJ, D'Alessandro AM, Knechtle SJ, Stegall MD, Pirsch JD, Hoffmann RM, et al. Risk factors for primary dysfunction after liver transplantation–a multivariate analysis. Transplantation 1993;55:807‐813. - PubMed
-
- Leithead JA, Tariciotti L, Gunson B, Holt A, Isaac J, Mirza DF, et al. Donation after cardiac death liver transplant recipients have an increased frequency of acute kidney injury. Am J Transplant 2012;12:965‐975. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
