

Rapidly Improving ARDS in Therapeutic Randomized Controlled Trials
- PMID: 30359616
- PMCID: PMC6414787
- DOI: 10.1016/j.chest.2018.09.031
Rapidly Improving ARDS in Therapeutic Randomized Controlled Trials
Abstract
Background: Observational studies suggest that some patients meeting criteria for ARDS no longer fulfill the oxygenation criterion early in the course of their illness. This subphenotype of rapidly improving ARDS has not been well characterized. We attempted to assess the prevalence, characteristics, and outcomes of rapidly improving ARDS and to identify which variables are useful to predict it.
Methods: A secondary analysis was performed of patient level data from six ARDS Network randomized controlled trials. We defined rapidly improving ARDS, contrasted with ARDS > 1 day, as extubation or a Pao2 to Fio2 ratio (Pao2:Fio2) > 300 on the first study day following enrollment.
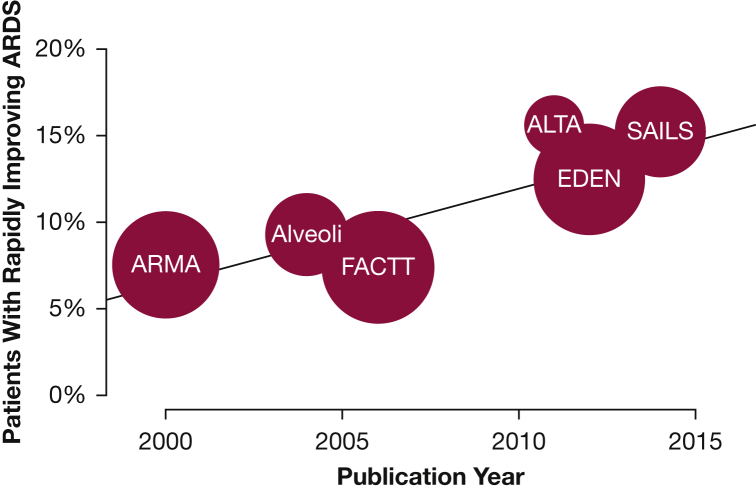
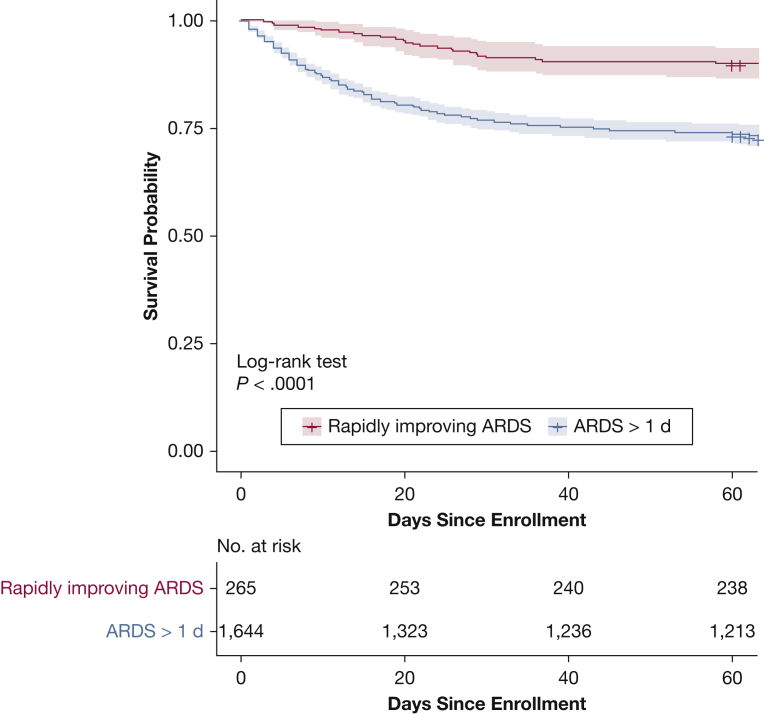
Results: The prevalence of rapidly improving ARDS was 10.5% (458 of 4,361 patients) and increased over time. Of the 1,909 patients enrolled in the three most recently published trials, 197 (10.3%) were extubated on the first study day, and 265 (13.9%) in total had rapidly improving ARDS. Patients with rapidly improving ARDS had lower baseline severity of illness and lower 60-day mortality (10.2% vs 26.3%; P < .0001) than ARDS > 1 day. Pao2:Fio2 at screening, change in Pao2:Fio2 from screening to enrollment, use of vasopressor agents, Fio2 at enrollment, and serum bilirubin levels were useful predictive variables.
Conclusions: Rapidly improving ARDS, mostly defined by early extubation, is an increasingly prevalent and distinct subphenotype, associated with better outcomes than ARDS > 1 day. Enrollment of patients with rapidly improving ARDS may negatively affect the prognostic enrichment and contribute to the failure of therapeutic trials.
Keywords: ICUs; acute lung injury; acute respiratory failure; epidemiology.
Copyright © 2018 American College of Chest Physicians. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Embracing the Heterogeneity of ARDS.Chest. 2019 Mar;155(3):453-455. doi: 10.1016/j.chest.2018.11.016. Chest. 2019. PMID: 30846060 No abstract available.
-
Heterogeneity of Acute Respiratory Distress Syndrome.Am J Respir Crit Care Med. 2020 Mar 15;201(6):728-730. doi: 10.1164/rccm.201906-1110RR. Am J Respir Crit Care Med. 2020. PMID: 31995400 No abstract available.
References
-
- Bellani G., Laffey J.G., Pham T. LUNG SAFE Investigators; ESICM Trials Group. Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA. 2016;315(8):788–800. - PubMed
-
- Fan E., Del Sorbo L., Goligher E.C. American Thoracic Society, European Society of Intensive Care Medicine, and Society of Critical Care Medicine. An official American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine clinical practice guideline: mechanical ventilation in adult patients with acute respiratory distress syndrome. Am J Respir Crit Care Med. 2017;195(9):1253–1263. - PubMed
-
- Reade M.C., Finfer S. Sedation and delirium in the intensive care unit. N Engl J Med. 2014;370(5):444–454. - PubMed
-
- Guérin C., Reignier J., Richard J.C., PROSEVA Study Group Prone positioning in severe acute respiratory distress syndrome. N Engl J Med. 2013;368(23):2159–2168. - PubMed
-
- Kor D.J., Carter R.E., Park P.K. US Critical Illness and Injury Trials Group: Lung Injury Prevention with Aspirin Study Group (USCIITG: LIPS-A). Effect of aspirin on development of ARDS in at-risk patients presenting to the emergency department: the LIPS—a randomized clinical trial. JAMA. 2016;315(22):2406–2414. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
