

Chronic venous insufficiency and varicose veins of the lower extremities
- PMID: 30360023
- PMCID: PMC6406103
- DOI: 10.3904/kjim.2018.230
Chronic venous insufficiency and varicose veins of the lower extremities
Abstract
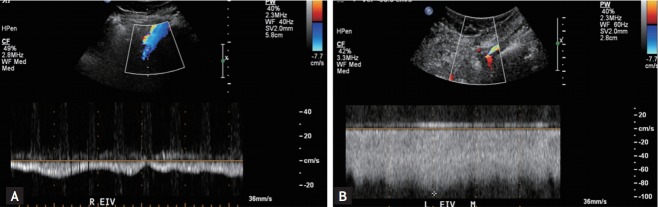
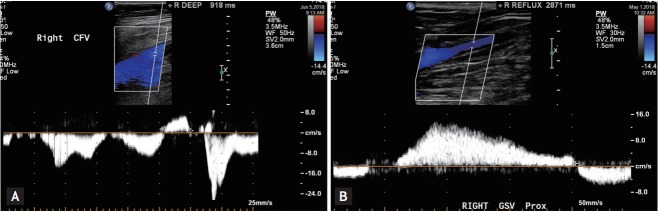
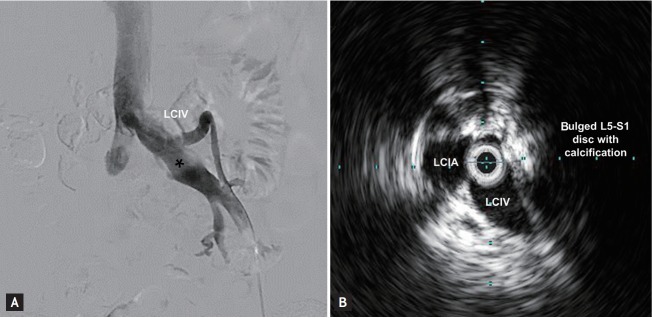
Chronic venous insufficiency (CVI) of the lower extremities manifests itself in various clinical spectrums, ranging from asymptomatic but cosmetic problems to severe symptoms, such as venous ulcer. CVI is a relatively common medical problem but is often overlooked by healthcare providers because of an underappreciation of the magnitude and impact of the problem, as well as incomplete recognition of the various presenting manifestations of primary and secondary venous disorders. The prevalence of CVI in South Korea is expected to increase, given the possible underdiagnoses of CVI, the increase in obesity and an aging population. This article reviews the pathophysiology of CVI of the lower extremities and highlights the role of duplex ultrasound in its diagnosis and radiofrequency ablation, and iliac vein stenting in its management.
Keywords: Diagnosis; Review; Therapeutics; Venous insufficiency.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
Similar articles
-
Unusual cause of pelvic congestion syndrome: Agenesis of the common and external iliac veins.J Med Vasc. 2021 Feb;46(1):32-34. doi: 10.1016/j.jdmv.2020.11.002. Epub 2020 Dec 10. J Med Vasc. 2021. PMID: 33546820 No abstract available.
-
Chronic venous disease.Minerva Cardioangiol. 2007 Aug;55(4):459-76. Minerva Cardioangiol. 2007. PMID: 17653022 Review. English, Italian. No abstract available.
-
Venous disorders: treatment with sclerosant foam.J Cardiovasc Surg (Torino). 2006 Feb;47(1):9-18. J Cardiovasc Surg (Torino). 2006. PMID: 16434941
-
Chronic Venous Insufficiency Evaluation and Medical Management.Curr Cardiol Rep. 2024 Nov;26(11):1241-1247. doi: 10.1007/s11886-024-02119-1. Epub 2024 Aug 31. Curr Cardiol Rep. 2024. PMID: 39215951 Review.
-
Clinical presentation and patterns of venous reflux in Thai patients with chronic venous insufficiency (CVI).Eur J Vasc Endovasc Surg. 2010 Sep;40(3):399-402. doi: 10.1016/j.ejvs.2010.04.017. Epub 2010 Jun 18. Eur J Vasc Endovasc Surg. 2010. PMID: 20561800
Cited by
-
Outcome of preventive nursing intervention, prophylactic anticoagulation and the use of the Caprini score on venous thromboembolism after varicose vein surgery.Afr Health Sci. 2023 Sep;23(3):616-623. doi: 10.4314/ahs.v23i3.72. Afr Health Sci. 2023. PMID: 38357111 Free PMC article.
-
Concentrations of selected acute phase proteins in patients with chronic venous insufficiency treated with Sulodexide. Part 1.Postepy Dermatol Alergol. 2023 Feb;40(1):126-133. doi: 10.5114/ada.2022.122605. Epub 2023 Feb 27. Postepy Dermatol Alergol. 2023. PMID: 36909895 Free PMC article.
-
Noncontrast MRI in assessing venous reflux of legs using QFlow analysis and radial basis function neural network technique.Sci Rep. 2023 Feb 24;13(1):3263. doi: 10.1038/s41598-023-30437-x. Sci Rep. 2023. PMID: 36828951 Free PMC article.
-
Preliminary application of three-dimensional venography and fusion navigation technique in May-Thurner syndrome.J Vasc Surg Venous Lymphat Disord. 2024 Jul;12(4):101660. doi: 10.1016/j.jvsv.2023.08.004. Epub 2023 Aug 10. J Vasc Surg Venous Lymphat Disord. 2024. PMID: 37572776 Free PMC article.
-
Rate of saphenous vein occlusion and side effects at 1 year follow up after 1470 nm endolaser.J Vasc Bras. 2023 Jul 21;22:e20210181. doi: 10.1590/1677-5449.202101812. eCollection 2023. J Vasc Bras. 2023. PMID: 37576737 Free PMC article.
References
-
- Raju S, Neglen P. Clinical practice. Chronic venous insufficiency and varicose veins. N Engl J Med. 2009;360:2319–2327. - PubMed
-
- Eberhardt RT, Raffetto JD. Chronic venous insufficiency. Circulation. 2014;130:333–346. - PubMed
-
- Santler B, Goerge T. Chronic venous insufficiency: a review of pathophysiology, diagnosis, and treatment. J Dts. - PubMed
-
- Callam MJ. Epidemiology of varicose veins. Br J Surg. 1994;81:167–173. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical