

Performance, Acceptability, and Usability of Respiratory Rate Timers and Pulse Oximeters When Used by Frontline Health Workers to Detect Symptoms of Pneumonia in Sub-Saharan Africa and Southeast Asia: Protocol for a Two-Phase, Multisite, Mixed-Methods Trial
- PMID: 30361195
- PMCID: PMC6231813
- DOI: 10.2196/10191
Performance, Acceptability, and Usability of Respiratory Rate Timers and Pulse Oximeters When Used by Frontline Health Workers to Detect Symptoms of Pneumonia in Sub-Saharan Africa and Southeast Asia: Protocol for a Two-Phase, Multisite, Mixed-Methods Trial
Erratum in
-
Metadata Correction: Performance, Acceptability, and Usability of Respiratory Rate Timers and Pulse Oximeters When Used by Frontline Health Workers to Detect Symptoms of Pneumonia in Sub-Saharan Africa and Southeast Asia: Protocol for a Two-Phase, Multisite, Mixed-Methods Trial.JMIR Res Protoc. 2019 Mar 7;8(3):e13755. doi: 10.2196/13755. JMIR Res Protoc. 2019. PMID: 30844745 Free PMC article.
Abstract
Background: Pneumonia is one of the leading causes of death in children aged under 5 years in both sub-Saharan Africa and Southeast Asia. The current diagnostic criterion for pneumonia is based on the increased respiratory rate (RR) in children with cough or difficulty breathing. Low oxygen saturation, measured using pulse oximeters, is indicative of severe pneumonia. Health workers often find it difficult to accurately count the number of breaths, and the current RR counting devices are often difficult to use or unavailable. Nonetheless, improved counting devices and low-cost pulse oximeters are now available on the market.
Objective: The objective of our study was to identify the most accurate, usable, and acceptable devices for the diagnosis of pneumonia symptoms by community health workers and first-level health facility workers or frontline health workers in resource-poor settings.
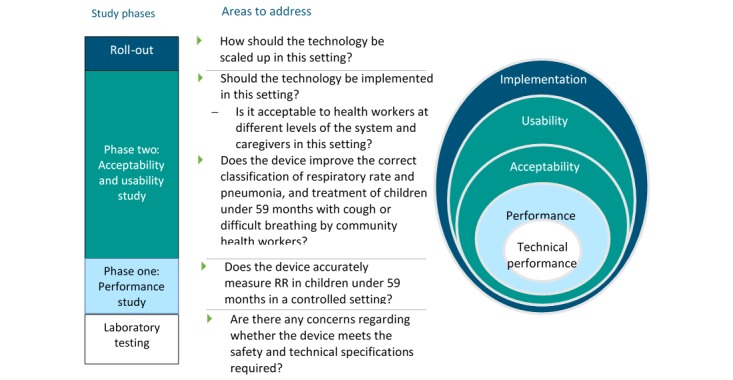
Methods: This was a multicenter, prospective, two-stage, observational study to assess the performance and usability or acceptability of 9 potential diagnostic devices when used to detect symptoms of pneumonia in the hands of frontline health workers. Notably, 188 possible devices were ranked and scored, tested for suitability in a laboratory, and 5 pulse oximeters and 4 RR timers were evaluated for usability and performance by frontline health workers in hospital, health facility, and community settings. The performance was evaluated against 2 references over 3 months in Cambodia, Ethiopia, South Sudan, and Uganda. Furthermore, acceptability and usability was subsequently evaluated using both qualitative and quantitative methodologies in routine practice, over 3 months, in the 4 countries.
Results: This project was funded in 2014, and data collection has been completed. Data analysis is currently under way, and the first results are expected to be submitted for publication in 2018.
Conclusions: This is the first large-scale evaluation of tools to detect symptoms of pneumonia at the community level. In addition, selecting an appropriate reference standard against which the devices were measured was challenging given the lack of existing standards and differences of opinions among experts. The findings from this study will help create a standardized and validated protocol for future studies and support further comparative testing of diagnostic devices in these settings.
Trial registration: Australian New Zealand Clinical Trials Registry ACTRN12615000348550; https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=367306&isReview=true (Archived by Website at http://www.webcitation.org/72OcvgBcf).
International registered report identifier (irrid): RR1-10.2196/10191.
Keywords: childhood pneumonia; diagnostic tools; low-income country; pulse oximeter; research design; respiratory rate counting.
©Kevin Baker, Mucunguzi Akasiima, Alexandra Wharton-Smith, Tedila Habte, Lena Matata, Diana Nanyumba, Morris Okwir, Anteneh Sebsibe, Madeleine Marasciulo, Max Petzold, Karin Källander. Originally published in JMIR Research Protocols (http://www.researchprotocols.org), 25.10.2018.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- Requejo J, Bryce J, Barros A, Berman P, Bhutta Z, Chopra M, Daelmans B, de Francisco A, Lawn J, Maliqi B, Mason E, Newby H, Presern C, Starrs A, Victora C. Countdown to 2015 and beyond: fulfilling the health agenda for women and children. The Lancet. 2015 Jan;385(9966):466–476. doi: 10.1016/S0140-6736(14)60925-9. - DOI - PMC - PubMed
-
- Bojalil R, Kirkwood BR, Bobak M, Guiscafre H. The relative contribution of case management and inadequate care-seeking behaviour to childhood deaths from diarrhoea and acute respiratory infections in Hidalgo, Mexico. Trop Med Int Health. 2007 Dec;12(12):1545–52. doi: 10.1111/j.1365-3156.2007.01963.x. doi: 10.1111/j.1365-3156.2007.01963.x.TMI1963 - DOI - PubMed
-
- WHO . WHO. Geneva: WHO; 2014. Revised WHO classification and treatment of childhood pneumonia at health facilities.
-
- Muro F, Mtove G, Mosha N, Wangai H, Harrison N, Hildenwall H, Schellenberg D, Todd J, Olomi R, Reyburn H. Effect of context on respiratory rate measurement in identifying non-severe pneumonia in African children. Trop Med Int Health. 2015 Jun;20(6):757–65. doi: 10.1111/tmi.12492. doi: 10.1111/tmi.12492. - DOI - PMC - PubMed
-
- Källander Karin, Tomson G, Nsabagasani X, Sabiiti J, Pariyo G, Peterson S. Can community health workers and caretakers recognise pneumonia in children? Experiences from western Uganda. Trans R Soc Trop Med Hyg. 2006 Oct;100(10):956–63. doi: 10.1016/j.trstmh.2005.11.004.S0035-9203(05)00430-X - DOI - PubMed
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
