

Case Reports
doi: 10.1259/bjrcr.20170091.
eCollection 2018.
Two cases of mimics of bone metastasis in breast cancer
Affiliations
- PMID: 30363150
- PMCID: PMC6159113
- DOI: 10.1259/bjrcr.20170091
Item in Clipboard
Case Reports
Two cases of mimics of bone metastasis in breast cancer
BJR Case Rep.
.
Abstract
In patients with breast cancer, the appearance of sclerotic bone lesions on imaging should raise the suspicion of skeletal metastases. However, before making the diagnosis it is important to consider the clinical context and remember that there are conditions that can mimic bone metastasis. We present two cases of mimics of bone metastasis: systemic mastocytosis and osteopoikilosis. These cases demonstrate clinical and radiological characteristics that would make a diagnosis of bone metastasis less likely, and highlight the need for an awareness of mimics of bone metastasis.
Figures

Additional imaging requested to investigate increased density in the lumbar spine on DEXA scan of a 57-year-old female with early-stage breast cancer (Case 1). (a) X-ray of lumbosacral spine showing focal bony sclerosis at T12 and L1. (b) Sagittal section of CT of lumbosacral spine showing sclerotic lesions in L1 to L4. (c) Sagittal T1 section of MRI of lumbosacral spine showing corresponding low signal lesions in the vertebral bodies.

Isotope bone scan for a 57-year-old female with early stage breast cancer (Case 1) showing subtle focal uptake in L1, possibly L3, left sacroiliac joint, left iliac bone and left acetabulum. There was surprisingly little uptake considering the X-ray appearances. Potential explanations provided for the relative lack of uptake on the bone scan were: inactive metastatic disease, perhaps in response to Letrozole; or an aggressive osteoclastic component masking uptake.

Isotope bone scan of a 50-year-old female with node-positive breast cancer (Case 2) showing subtle increased uptake in the left anterior chest consistent with recent breast surgery but no evidence of bone metastases.

X-ray of pelvis of a 50-year-old female with node-positive breast cancer (Case 2) showing multiple sclerotic lesions in the iliac wings and proximal femora.
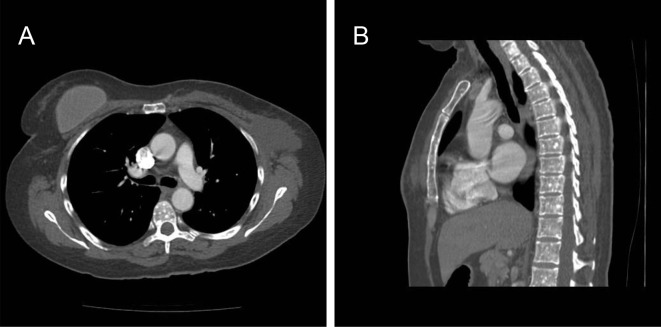
CT scan of a 50-year-old female with node-positive breast cancer (Case 2). (a) Axial CT image of the thorax showing multiple, small, rounded sclerotic foci in the T7 vertebral body. (b) Sagittal CT image showing multiple, small, rounded, sclerotic lesions throughout the vertebra and sternum.
References
-
- Pavlakis N, Schmidt R, Stockler M.. Bisphosphonates for breast cancer. Cochrane Database Syst Rev 2005; 20. - PubMed
-
- Andersen CL, Kristensen TK, Severinsen MT, Møller MB, Vestergaard H, Bergmann OJ, et al. Systemic mastocytosis--a systematic review. Dan Med J 2012; 59: A4397–402. - PubMed
-
- Horny H, Akin C, Metcalfe D. et al. WHO claddification of tumours of haematopoietic and lymphoid origin : Swedlow SH. . Mastocytosis. Lyon: IARC; 2008. 54–63
-
- Jangir RR, et al. Osteopoikilosis and its clinical significance: a review of the literature. Research and Reviews. Journal of Medical and Health Sciences, 2014; 3: 11–20.
-
- Metcalfe DD, Baram D, Mekori YA.. Mast cells. Physiol Rev 1997; 77: 1033–79. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
