

Role of PET imaging for biochemical recurrence following primary treatment for prostate cancer
- PMID: 30363475
- PMCID: PMC6178324
- DOI: 10.21037/tau.2018.06.09
Role of PET imaging for biochemical recurrence following primary treatment for prostate cancer
Abstract
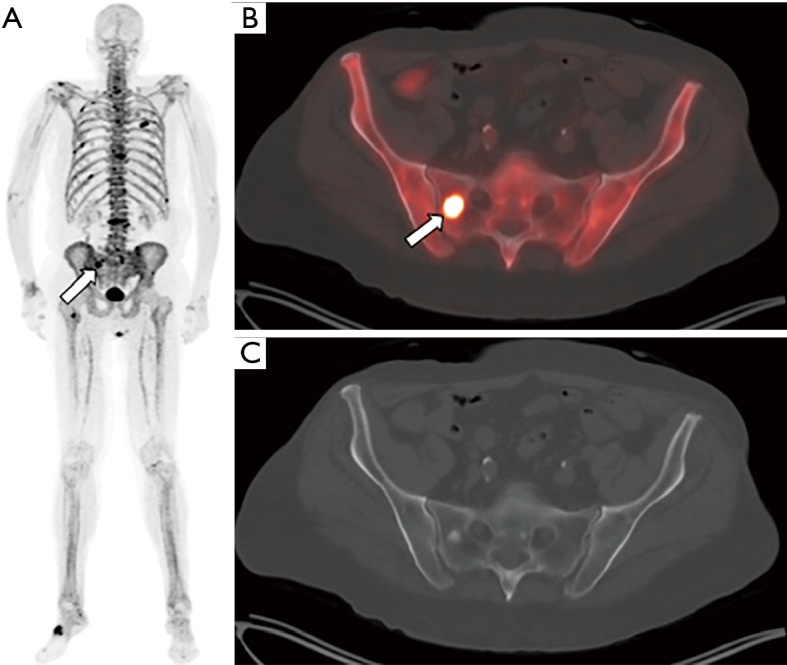
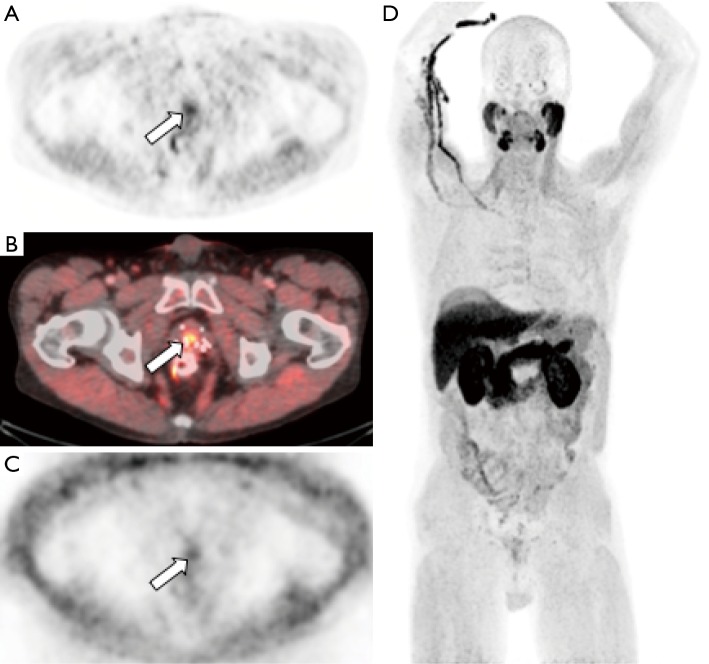
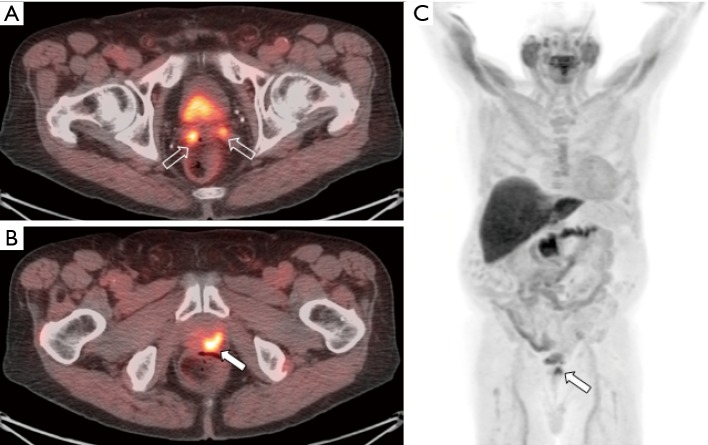
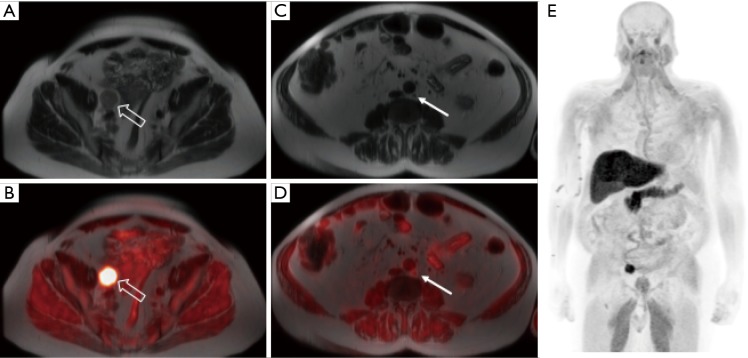
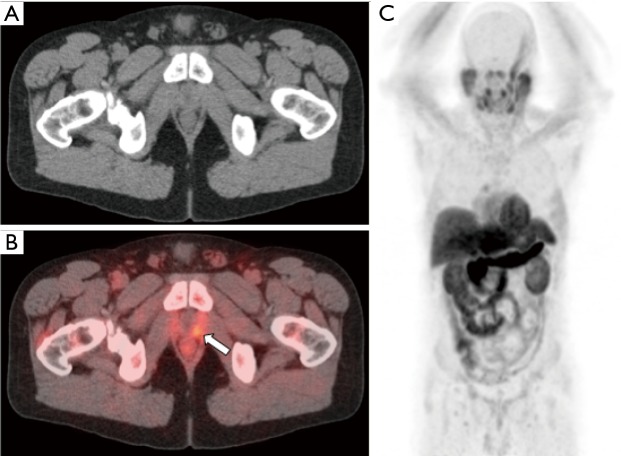
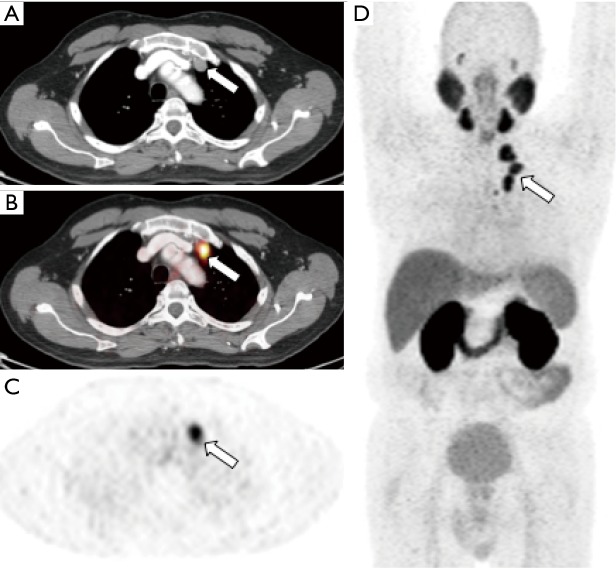
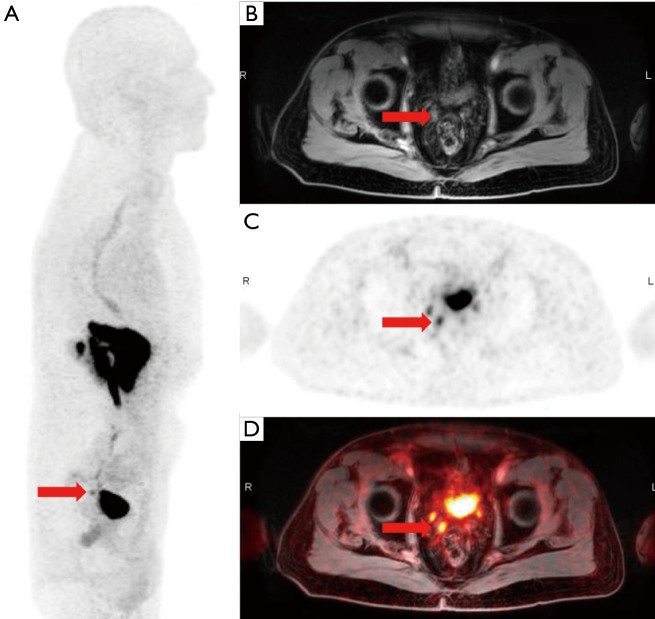
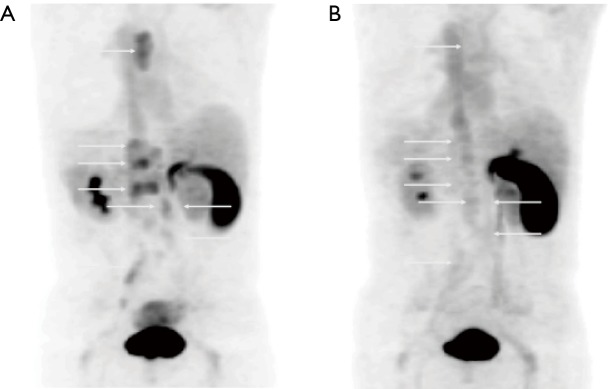
Prostate cancer is one of the most common cancers in men worldwide, and primary prostate cancer is typically treated with surgery, radiation, androgen deprivation, or a combination of these therapeutic modalities. Despite technical advances, approximately 30% of men will experience biochemical recurrent within 10 years of definitive treatment. Upon detection of a rise in serum prostate specific antigen (PSA), there is great need to accurately stage these patients to help guide further therapy. As a result, there are considerable efforts underway to establish the role of positron emission tomography (PET) in the diagnostic algorithm of biochemically recurrent prostate cancer. This manuscript provides an overview of PET tracers used for the detection and localization of prostate cancer in the setting of biochemical recurrence with a focus on PET tracers that are currently being used in clinical practice in the United States.
Keywords: Biochemical recurrence; PET/magnetic resonance imaging (MRI); positron emission tomography (PET)/computed tomography (CT); prostate cancer.
Conflict of interest statement
Conflicts of Interest: Drs. Galgano and McConathy receive research support from Blue Earth Diagnostics. Dr. Valentin has no conflicts of interest to declare.
Figures
References
-
- Global Burden of Disease Cancer Collaboration , Fitzmaurice C, Allen C, et al. Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived With Disability, and Disability-Adjusted Life-years for 32 Cancer Groups, 1990 to 2015: A Systematic Analysis for the Global Burden of Disease Study. JAMA Oncol 2017;3:524-48. 10.1001/jamaoncol.2016.5688 - DOI - PMC - PubMed
-
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Prostate Cancer Version 2.2018. June 3, 2018; Available online: https://www.nccn.org/professionals/physician_gls/PDF/prostate.pdf
-
- Roehl KA, Han M, Ramos CG, et al. Cancer progression and survival rates following anatomical radical retropubic prostatectomy in 3,478 consecutive patients: long-term results. J Urol 2004;172:910-4. 10.1097/01.ju.0000134888.22332.bb - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous