

Complicated acute haematogenous osteomyelitis with fatal outcome following a closed clavicle fracture-a case report and literature review
- PMID: 30363605
- PMCID: PMC6180849
- DOI: 10.1259/bjrcr.20150389
Complicated acute haematogenous osteomyelitis with fatal outcome following a closed clavicle fracture-a case report and literature review
Abstract
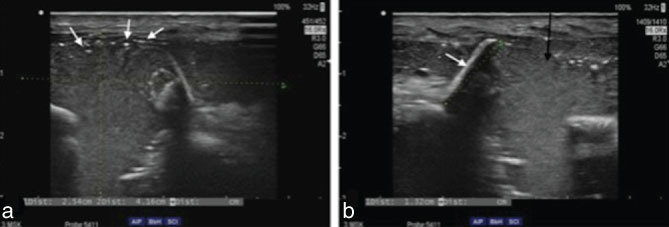
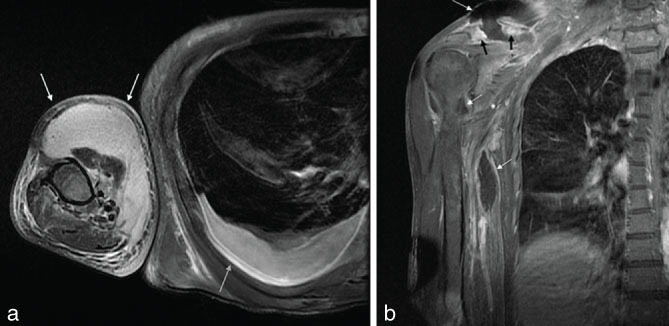
Among adults, post-traumatic osteomyelitis following a closed fracture is a rarely described entity in the literature, with the involvement of the clavicle bone being particularly uncommon. Early diagnosis and treatment of clavicular osteomyelitis is crucial to prevent serious consequences such as sepsis, mediastinitis and haemorrhage from the great vessels. A 54-year-old male patient presented to the emergency department complaining of fatigue and limited mobility after having fallen and hit his head and right shoulder 10 days previously. No major injury was found during the diagnostic procedure, and the patient was discharged. 2 weeks later, the patient returned with clinical signs of right upper arm cellulitis and probable sepsis. Diagnostic ultrasound imaging and MRI of the right upper arm, as well as re-examination of the X-ray image, confirmed acute complex osteomyelitis of the right clavicle following an overlooked clavicle fracture. Microbiological analysis confirmed clavicular osteomyelitis caused by Escherichia coli septicaemia. Despite prompt treatment with i.v. antibiotics and surgery, the patient's condition rapidly deteriorated and he passed away. Our case demonstrates the critical importance of early diagnosis and appropriate treatment of a closed fracture. Late diagnosis may lead to severe complications, such as complicated osteomyelitis and sepsis, and even a fatal outcome. Furthermore, a brief literature review is presented of previously reported acute osteomyelitis following a closed fracture, including evidence of affected bone and isolated pathogens. Although uncommon, osteomyelitis should be considered a possible cause of a deteriorating clinical condition in patients with a history of recent trauma.
Figures

References
-
- Waldvogel FA, Medoff G, Swartz MN. Osteomyelitis: a review of clinical features, therapeutic considerations and unusual aspects. N Engl J Med 1970; 282: 198–206. - PubMed
-
- Sonobe M, Miyazaki M, Nakagawa M, Ikegami N, Suzumura Y, Nagasawa M, et al. Descending necrotizing mediastinitis with sternocostoclavicular osteomyelitis and partial thoracic empyema: report of a case. Surg Today 1999; 29: 1287–9. - PubMed
-
- Cremieux AC, Carbon C. Experimental models of bone and prosthetic joint infections. Clin Infect Dis 1997; 25: 1295–302. - PubMed
-
- Norden CW. Bone and joint infection. Curr Opin Infect Dis 1996; 9: 109–14.
Publication types
LinkOut - more resources
Full Text Sources
