

Current Concepts in the Treatment of Multiple System Atrophy
- PMID: 30363880
- PMCID: PMC6183186
- DOI: 10.1002/mdc3.12145
Current Concepts in the Treatment of Multiple System Atrophy
Abstract
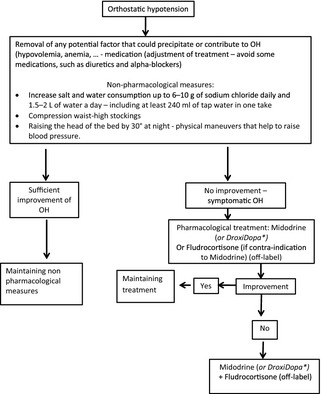
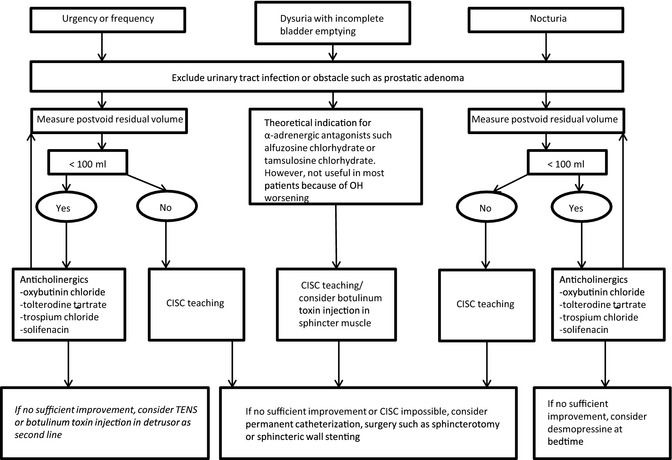
MSA is a progressive neurodegenerative disorder characterized by autonomic failure and a variable combination of poor levodopa-responsive parkinsonism and cerebellar ataxia (CA). Current therapeutic management is based on symptomatic treatment. Almost one third of MSA patients may benefit from l-dopa for the symptomatic treatment of parkinsonism, whereas physiotherapy remains the best therapeutic option for CA. Only midodrine and droxidopa were found to be efficient for neurogenic hypotension in double-blind, controlled studies, whereas other symptoms of autonomic failure may be managed with off-label treatments. To date, no curative treatment is available for MSA. Recent results of neuroprotective and -restorative trials have provided some hope for future advances. Considerations for future clinical trials are also discussed in this review.
Keywords: ataxia; atypical parkinsonism; autonomic dysfunction; multiple system atrophy; treatment.
Figures
References
-
- Tison F, Yekhlef F, Chrysostome V, et al. Parkinsonism in multiple system atrophy: natural history, severity (UPDRS‐III), and disability assessment compared with Parkinson's disease. Mov Disord 2002;17:701–709. - PubMed
-
- Schrag A, Geser F, Stampfer‐Kountchev M, et al. Health‐related quality of life in multiple system atrophy. Mov Disord 2006;21:809–815. - PubMed
-
- Watanabe H, Saito Y, Terao S, et al. Progression and prognosis in multiple system atrophy: an analysis of 230 Japanese patients. Brain 2002;125(Pt 5):1070–1083. - PubMed
-
- Schrag A, Wenning GK, Quinn N, Ben‐Shlomo Y. Survival in multiple system atrophy. Mov Disord 2008;23:294–296. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
