

Laparoscopic sphincter-saving surgery for low rectal cancer through marker meeting approach
- PMID: 30363998
- PMCID: PMC6186979
- DOI: 10.21037/atm.2018.08.02
Laparoscopic sphincter-saving surgery for low rectal cancer through marker meeting approach
Abstract
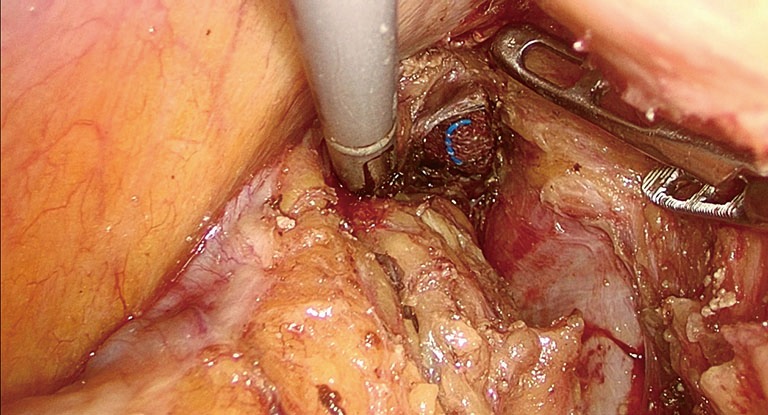
Laparoscopic low anterior resection (LAR) with sphincter preservation for ultra-low rectal cancer is always a challenging operation in colorectal surgery. To achieve negative margins, reducing the difficulty and risks of the procedure are major goals for us. The marker meeting approach we reported can help to accomplish this goal. The key technique for the marker meeting approach is to ensure a clear distal margin in a low resection of the rectum by transanal dissection. This procedure allows access to the space around the distal rectum and mesorectum and to pack the gauzes in the distal part of the space as a landmark. Routine laparoscopic LAR was performed to dissect the space until reaching the gauzes packed above and achieve complete mobilization of the rectum and mesorectum. This surgical procedure is simpler and reduces the difficulty of the operation. Therefore, it is expected to reduce the risk of surgery-related complications and positive margins and is suitable to be widely applied and extended in clinical practice. The short-term and long-term clinical outcomes of the marker meeting approach need more research in large samples.
Keywords: Low rectal cancer; laparoscopic low anterior resection (laparoscopic LAR); marker meeting; total mesorectal excision (TME).
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures









References
-
- Guillou PJ, Quirke P, Thorpe H, et al. MRC CLASICC trial group. Short-term endpoints of conventional versus laparoscopic-assisted surgery in patients with colorectal cancer (MRC CLASICC trial): multicentre, randomised controlled trial. Lancet 2005; 365:1718-26. 10.1016/S0140-6736(05)66545-2 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous