

Treatment of Diabetic Macular Edema with Intravitreal Antivascular Endothelial Growth Factor and Prompt versus Deferred Focal Laser during Long-Term Follow-Up and Identification of Prognostic Retinal Markers
- PMID: 30364034
- PMCID: PMC6188720
- DOI: 10.1155/2018/3082560
Treatment of Diabetic Macular Edema with Intravitreal Antivascular Endothelial Growth Factor and Prompt versus Deferred Focal Laser during Long-Term Follow-Up and Identification of Prognostic Retinal Markers
Abstract
Purpose: Long-term follow-up of patients with diabetic macular edema (DME) treated with intravitreal antivascular endothelial growth factor (anti-VEGF) combined focal laser and identification of prognostic morphological characteristics.
Methods: Prospective clinical trial (50 treatment-naive eyes) with DME randomized 1 : 1 receiving intravitreal ranibizumab (0.5 mg/0.05 ml) and prompt grid laser compared with ranibizumab and deferred laser. Morphological characteristics potentially relevant for prognosis were assessed at baseline, month 6, month 9, and years 1, 2, 3, 4, and 5 of follow-up.
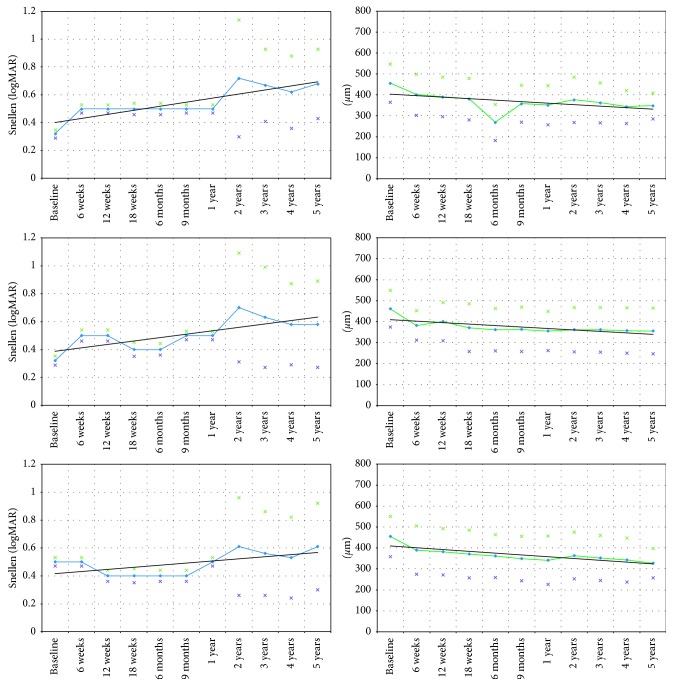
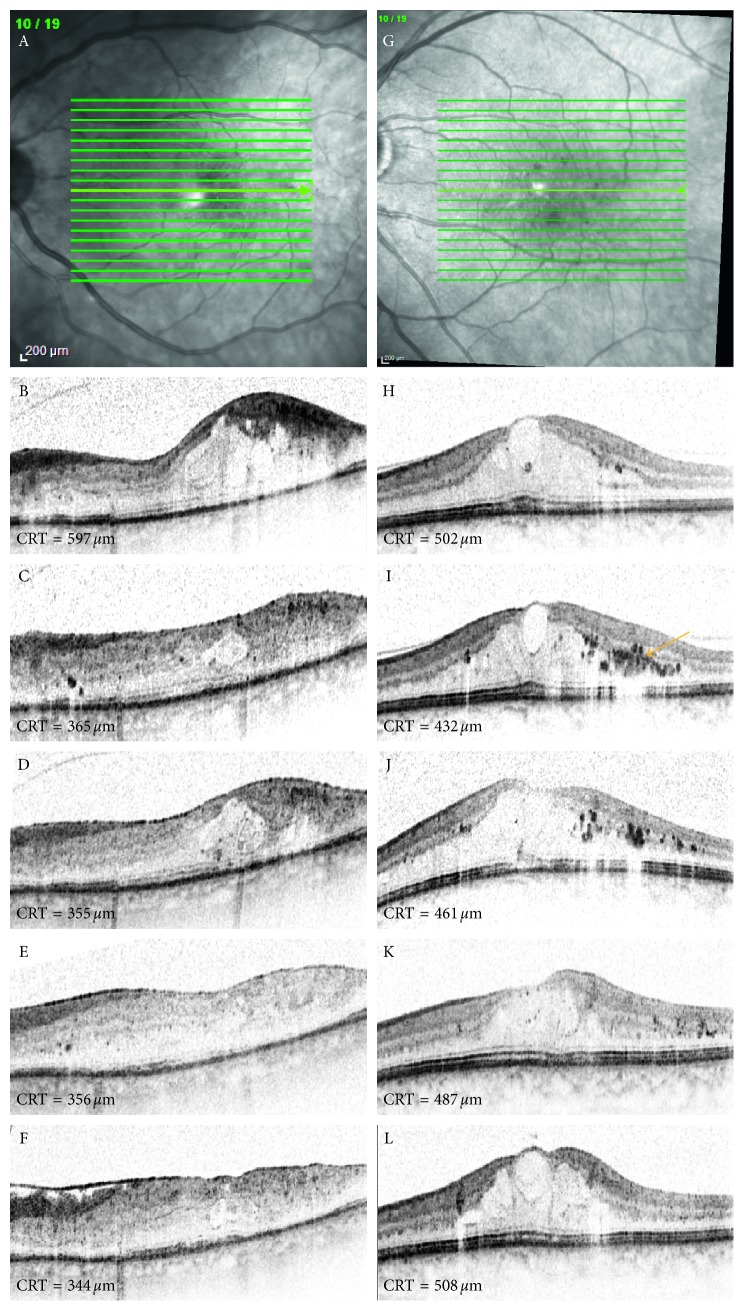
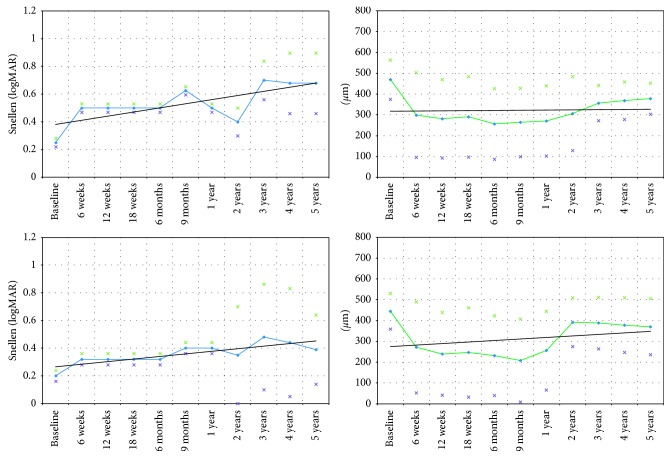
Results: Although functional results were slightly higher in the prompt group at week 12 (0.5; 20/40 Snellen (SD = 0.04, 0.3 logMAR) versus 0.4; 20/50 Snellen (SD = 0.04, logMAR: 0.4), p=0.4) and month 9 (prompt group: 0.5; 20/40 Snellen (SD = 0.03, 0.3 logMAR) versus deferred group: 0.4; 20/50 Snellen (SD = 0.04, 0.4 logMAR), p=0.4), these were statistically insignificant. There was no significant benefit regarding functionality during long-term follow-up in the prompt group compared to the deferred group. BCVA in the eyes with clusters of hyperreflective foci in the central macular region was inferior compared with the eyes without these alterations at year 5 (0.39; 20/50 Snellen, (SD = 0.25, 0.4 logMAR) versus 0.63; 20/80 Snellen (SD = 0.22, 0.2 logMAR), p < 0.01).
Conclusion: Grid laser and ranibizumab therapy are effective in DME management during the long-term follow-up. Intraretinal hyperreflective material in SD-OCT is negatively related to BCVA.
Figures
References
-
- Nathan D. M., Genuth S., Lachin J., et al. Photocoagulation therapy for diabetic eye disease: Early Treatment Diabetic Retinopathy Study Research Group. JAMA. 1985;254(21):3086–3087. - PubMed
LinkOut - more resources
Full Text Sources
