

The Association between Antihypertensive Medication Use and Blood Pressure Is Influenced by Obesity
- PMID: 30364090
- PMCID: PMC6188586
- DOI: 10.1155/2018/4573258
The Association between Antihypertensive Medication Use and Blood Pressure Is Influenced by Obesity
Abstract
Introduction: One in three US adults is living with obesity or hypertension, and more than 75% of hypertensive individuals are using antihypertensive medications. Therefore, it is important to examine blood pressure (BP) differences in populations that are using these medications with differing obesity status.
Aim: We examined whether BP attained when using various antihypertensive medications varies amongst different body mass index (BMI) categories and whether antihypertensive medication use is associated with differences in other metabolic risk factors, independent of BMI.
Methods: Adults with hypertension from the National Health and Nutrition Examination Survey (NHANES) from 1999 to 2014 were used (n=15,285). Linear regression analyses were used to examine the main effects and interaction between antihypertensive use and BMI.
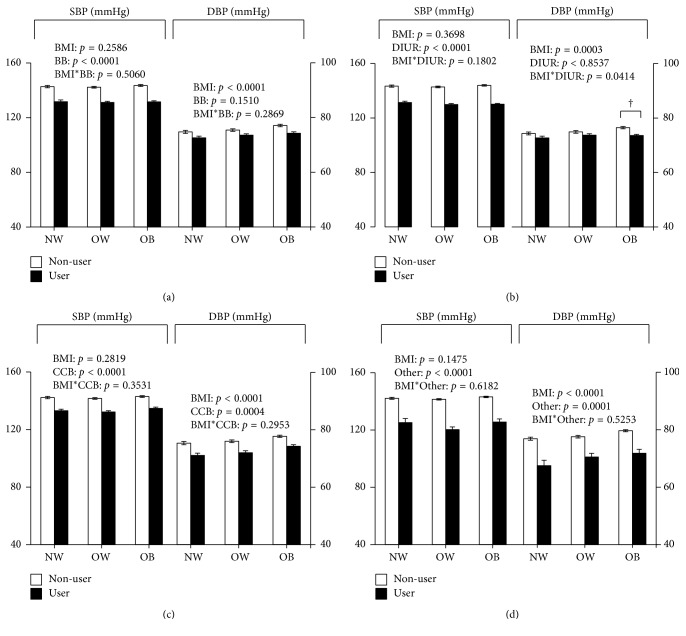
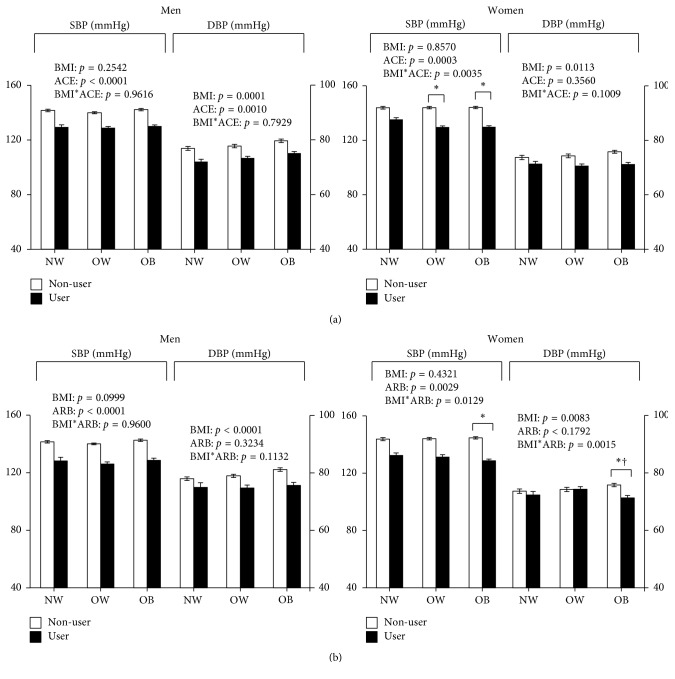
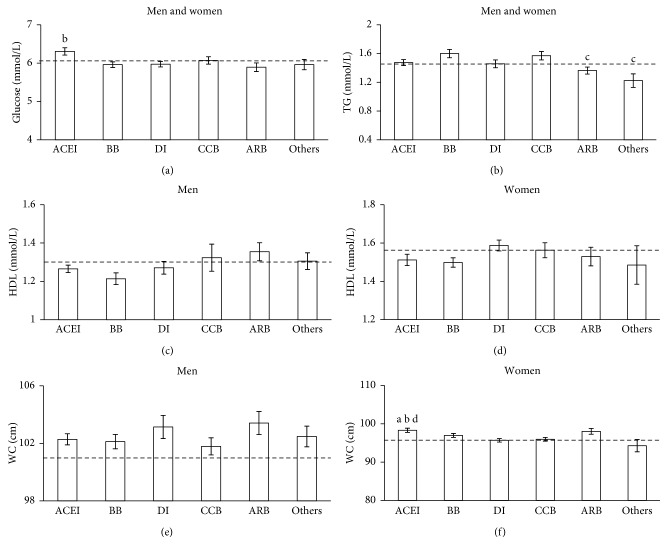
Results: In general, users of antihypertensive medications had lower BP than those not taking BP medications (NoBPMed) (P < 0.05), whereby in women, the differences in systolic BP between angiotensin-converting-enzyme (ACE) inhibitor or angiotensin receptor blocker (ARB) users and NoBPMed were greater in those with obesity (ACE inhibitors: -14 ± 1 mmHg; ARB: -16 ± 1 mmHg) compared to normal weight individuals (ACE inhibitors: -9 ± 1 mmHg; ARB: -11 ± 1 mmHg) (P < 0.05). Diastolic BP differences between women ARB users and NoBPMed were also greatest in obesity (-5 ± 1 mmHg) (P < 0.05) whilst there were no differences in normal weight individuals (-1 ± 1 mmHg) (P>0.05). Furthermore, glucose levels and waist circumference in women were higher in those using ACE inhibitors compared to diuretics (P < 0.05).
Conclusion: ACE inhibitors and ARBs may be associated with more beneficial BP profiles in women with obesity, with no obesity-related BP differences for antihypertensive medication in men. However, there could be potential cardiometabolic effects for some antihypertensive medications that should be explored further.
Figures
Similar articles
-
[Assessment of antihypertensive monotherapies effectiveness by home blood pressure self-measurement in hypertensive patients].Ann Cardiol Angeiol (Paris). 2012 Jun;61(3):218-23. doi: 10.1016/j.ancard.2012.05.002. Epub 2012 May 23. Ann Cardiol Angeiol (Paris). 2012. PMID: 22695025 French.
-
[Profile on circadian blood pressure and the influencing factors in essential hypertensive patients after treatment].Zhonghua Liu Xing Bing Xue Za Zhi. 2004 Aug;25(8):710-4. Zhonghua Liu Xing Bing Xue Za Zhi. 2004. PMID: 15555399 Chinese.
-
Usefulness of the alpha1-blocker doxazosin as a third-line antihypertensive drug.Hypertens Res. 2007 Apr;30(4):301-6. doi: 10.1291/hypres.30.301. Hypertens Res. 2007. PMID: 17541208 Clinical Trial.
-
Effects of renin-angiotensin system inhibition on end-organ protection: can we do better?Clin Ther. 2007 Sep;29(9):1803-24. doi: 10.1016/j.clinthera.2007.09.019. Clin Ther. 2007. PMID: 18035185 Review.
-
Administration-time differences in effects of hypertension medications on ambulatory blood pressure regulation.Chronobiol Int. 2013 Mar;30(1-2):280-314. doi: 10.3109/07420528.2012.709448. Epub 2012 Oct 19. Chronobiol Int. 2013. PMID: 23077971 Review.
Cited by
-
Angiotensin-(1-7) and Central Control of Cardiometabolic Outcomes: Implications for Obesity Hypertension.Int J Mol Sci. 2024 Dec 12;25(24):13320. doi: 10.3390/ijms252413320. Int J Mol Sci. 2024. PMID: 39769086 Free PMC article. Review.
-
Predicting of factors associated with valsartan response among hypertensive patients attending the Jordan University Hospital.Drug Metab Pers Ther. 2025 Feb 6;40(1):69-75. doi: 10.1515/dmpt-2024-0088. eCollection 2025 Mar 1. Drug Metab Pers Ther. 2025. PMID: 39909828
-
Effect of Angiotensin Receptor Blocker and Angiotensin Converting Enzyme Inhibitor on Kidney Function and Blood Potassium Level in Indonesian Type 2 Diabetes Mellitus with Hypertension: A Three-Month Cohort Study.Diabetes Metab Syndr Obes. 2021 Sep 7;14:3841-3849. doi: 10.2147/DMSO.S310091. eCollection 2021. Diabetes Metab Syndr Obes. 2021. PMID: 34522111 Free PMC article.
References
-
- American Heart Association. Heart Disease and Stroke Statistics 2018 At-a-Glance. Dallas, Texas, United States: American Heart Association; 2018. https://healthmetrics.heart.org/wp-content/uploads/2018/02/At-A-Glance-H....
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
