

Improving quality of care during childbirth in primary health centres: a stepped-wedge cluster-randomised trial in India
- PMID: 30364301
- PMCID: PMC6195146
- DOI: 10.1136/bmjgh-2018-000907
Improving quality of care during childbirth in primary health centres: a stepped-wedge cluster-randomised trial in India
Abstract
Background: Low/middle-income countries need a large-scale improvement in the quality of care (QoC) around the time of childbirth in order to reduce high maternal, fetal and neonatal mortality. However, there is a paucity of scalable models.
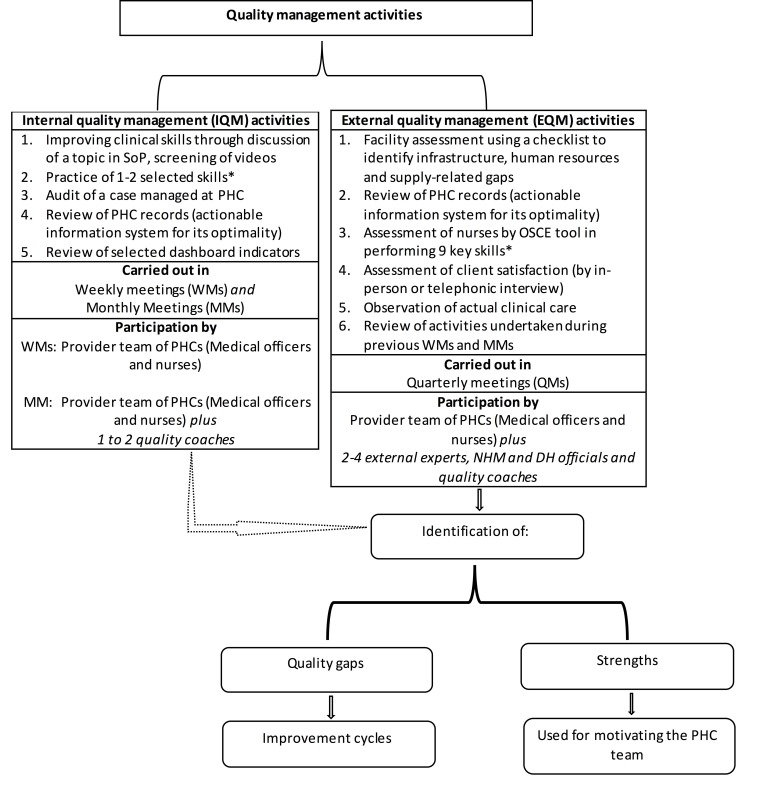
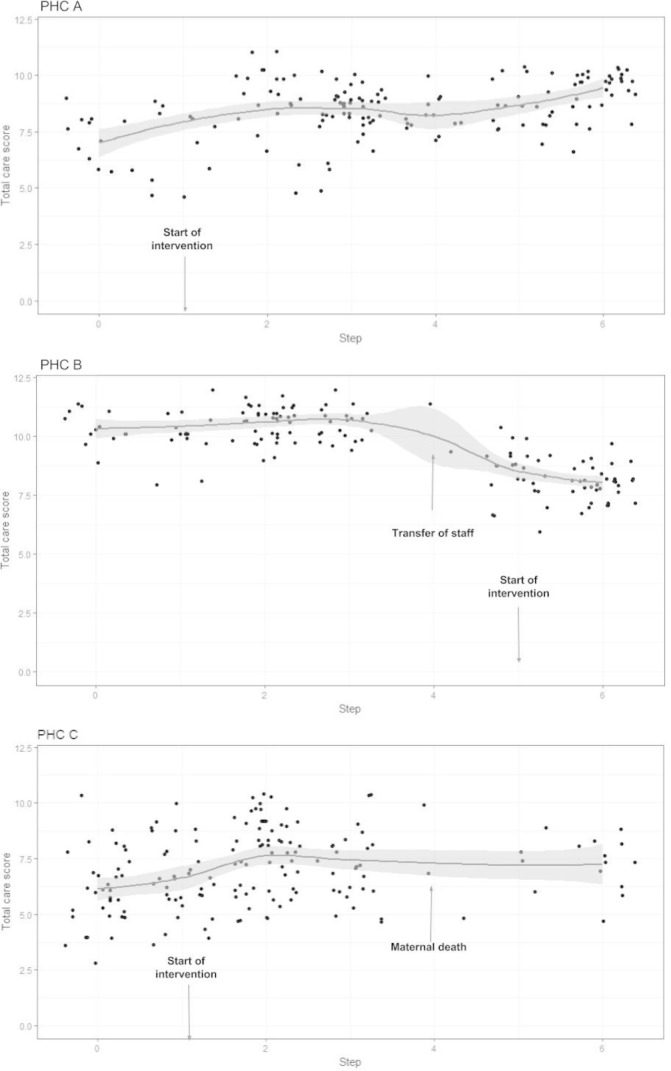
Methods: We conducted a stepped-wedge cluster-randomised trial in 15 primary health centres (PHC) of the state of Haryana in India to test the effectiveness of a multipronged quality management strategy comprising capacity building of providers, periodic assessments of the PHCs to identify quality gaps and undertaking improvement activities for closure of the gaps. The 21-month duration of the study was divided into seven periods (steps) of 3 months each. Starting from the second period, a set of randomly selected three PHCs (cluster) crossed over to the intervention arm for rest of the period of the study. The primary outcomes included the number of women approaching the PHCs for childbirth and 12 directly observed essential practices related to the childbirth. Outcomes were adjusted with random effect for cluster (PHC) and fixed effect for 'months of intervention'.
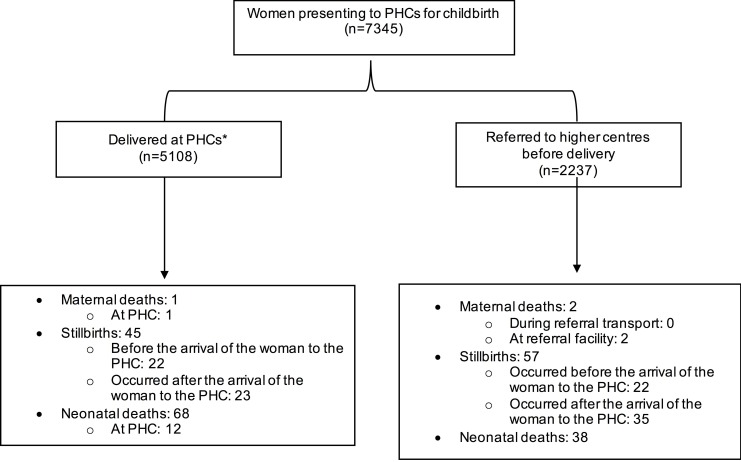
Results: The intervention strategy led to increase in the number of women approaching PHCs for childbirth (26 vs 21 women per PHC-month, adjusted incidence rate ratio: 1.22; 95% CI 1.17 to 1.28). Of the 12 practices, 6 improved modestly, 2 remained near universal during both intervention and control periods, 3 did not change and 1 worsened. There was no evidence of change in mortality with a majority of deaths occurring either during referral transport or at the referral facilities.
Conclusion: A multipronged quality management strategy enhanced utilisation of services and modestly improved key practices around the time of childbirth in PHCs in India.
Trial registration number: CTRI/2016/05/006963.
Keywords: cluster-randomised trial; health systems; maternal health; paediatrics.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- GBD 2015 Child Mortality Collaborators. Global, regional, national, and selected subnational levels of stillbirths, neonatal, infant, and under-5 mortality, 1980-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016;388:1725–74. 10.1016/S0140-6736(16)31575-6 - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources