

Acute massive congestive ischaemic colitis related to inferior mesenteric arteriovenous malformation
- PMID: 30364461
- PMCID: PMC6195917
- DOI: 10.1259/bjrcr.20150275
Acute massive congestive ischaemic colitis related to inferior mesenteric arteriovenous malformation
Abstract
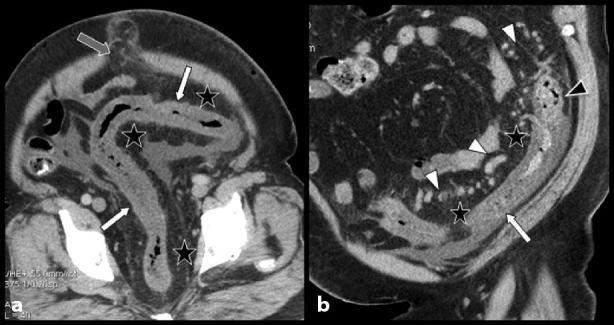
We report a very rare case of acute congestive ischaemic colitis of the left colon caused by brutal decompensation of an uncommon arteriovenous malformation (AVM) in the territory of the inferior mesenteric artery (IMA) in a 45-year-old male patient. The patient presented with severe abdominal pain in the left iliac fossa and abundant mucoid stools. The diagnosis of congestive colitis was made by optical colonoscopy but the full diagnosis of the responsible AVM in the IMA territory was made by contrast-enhanced multidetector CT scan combined with colour Doppler ultrasound. Two successive attempts at selective embolization failed to resolve the symptoms and finally, extensive surgery was necessary. The complete imaging findings of the case are presented and the characteristic features of uncommon AVMs and fistulas of the IMA territory are briefly reviewed.
Figures





References
-
- Metcalf DR, Nivatvongs S, Andrews JC. Ischemic colitis: an unusual case of inferior mesenteric arteriovenous fistula causing venous hypertension. Report of a case. Dis Colon Rectum 2008; 51: 1422–4. - PubMed
-
- Justaniah AI, Molgaard C, Flacke S, Barto A, Iqbal S. Congenital inferior mesenteric arteriovenous malformation presenting with ischemic colitis: endovascular treatment. J Vasc Interv Radiol 2013; 24: 1761–3. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
