

Self-report versus electronic medical record recorded healthcare utilisation in older community-dwelling adults: Comparison of two prospective cohort studies
- PMID: 30365518
- PMCID: PMC6203362
- DOI: 10.1371/journal.pone.0206201
Self-report versus electronic medical record recorded healthcare utilisation in older community-dwelling adults: Comparison of two prospective cohort studies
Abstract
Introduction: Self-reported measures of healthcare utilisation are often used in longitudinal cohort studies involving older community-dwelling people. The aim of this study is to compare healthcare utilisation rates using patient self-report and manual extraction from the general practice (GP) electronic medical record (EMR).
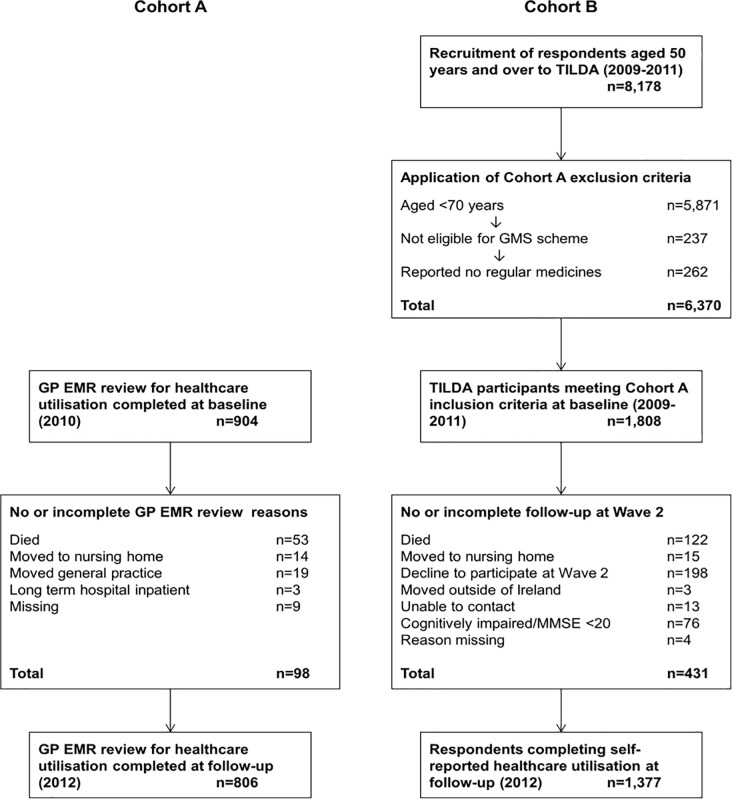
Methods: Study population: Two prospective cohort studies (n = 806 and n = 1,377, aged ≥70 years) conducted in the Republic of Ireland were compared. Study outcomes: GP, outpatient department (OPD) and emergency department (ED) visits over a one-year period. Statistical analysis: Descriptive statistics of the two cohorts are presented. A negative binomial regression was performed and results are presented as incidence rate ratios (IRR) with 95% confidence intervals (CI). For the outcome of any ED visit, linear regression was performed, yielding risk ratios (RR) with 95% CI.
Results: The annual rates of GP, OPD and ED visits were 6.30 (SD 4.63), 2.11 (SD 2.46) and 0.26 (SD 0.62) respectively in GP EMR cohort, compared to 5.65 (SD 8.06), 2.09 (SD 5.83) and 0.32 (SD 0.84) in the self-report cohort. In univariate regression analysis comparing healthcare utilisation, the self-report cohort reported a lower frequency of GP visits (unadjusted IRR 0.90 (95% CI 0.84, 0.96), p = 0.02)), a greater frequency of ED visits (1.20 (0.98, 1.49), p = 0.083)), and no difference in OPD visits (unadjusted IRR 0.99 (95% CI 0.86, 1.13), p = 0.845)). In multivariate analysis, adjusted for relevant confounders, there was no difference in GP visits (adjusted IRR 0.99 (95% CI 0.92, 1.06), p = 0.684)) or OPD visits (adjusted IRR 1.09 (0.95, 1.25), p = 0.23)) between the two cohorts. However, the self-report cohort reported 37% more ED visits (adjusted IRR 1.37 (1.10, 1.71), p = 0.005)) and were more likely to report any ED visit (adjusted RR 1.23 (95% CI 1.02, 1.48), p = 0.028)).
Conclusions: This study demonstrates that reported rates of GP and OPD visits were similar but there were differences in reported ED visits, with significantly higher self-reported visits. This may be due to ED visits not being notified to the GP and contextual issues such as transfer of healthcare utilisation data between sectors may vary in different healthcare systems.
Conflict of interest statement
The authors declare funding from the Health Research Board under grant HRC-2014-1 (TF), Irish Life (commercial funder), The Atlantic Philanthropies, and the Department of Health in Ireland (RAK). The funders, including the commercial funder Irish Life, had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
Similar articles
-
Association between adherence to antihypertensive medications and health outcomes in middle and older aged community dwelling adults; results from the Irish longitudinal study on ageing.Eur J Clin Pharmacol. 2019 Sep;75(9):1283-1292. doi: 10.1007/s00228-019-02699-w. Epub 2019 Jun 12. Eur J Clin Pharmacol. 2019. PMID: 31190134
-
Potentially inappropriate prescribing and its association with health outcomes in middle-aged people: a prospective cohort study in Ireland.BMJ Open. 2017 Oct 16;7(10):e016562. doi: 10.1136/bmjopen-2017-016562. BMJ Open. 2017. PMID: 29042380 Free PMC article.
-
The impact of stroke, cognitive function and post-stroke cognitive impairment (PSCI) on healthcare utilisation in Ireland: a cross-sectional nationally representative study.BMC Health Serv Res. 2022 Mar 29;22(1):414. doi: 10.1186/s12913-022-07837-2. BMC Health Serv Res. 2022. PMID: 35351125 Free PMC article.
-
Emergency department factors associated with survival after sudden cardiac arrest.Resuscitation. 2013 Mar;84(3):292-7. doi: 10.1016/j.resuscitation.2012.10.013. Epub 2012 Oct 24. Resuscitation. 2013. PMID: 23103887 Review.
-
Healthcare utilisation in overweight and obese children: a systematic review and meta-analysis.BMJ Open. 2020 Oct 8;10(10):e035676. doi: 10.1136/bmjopen-2019-035676. BMJ Open. 2020. PMID: 33033082 Free PMC article.
Cited by
-
Health care utilization and the associated costs attributable to cardiovascular disease in Ireland: a cross-sectional study.Eur Heart J Qual Care Clin Outcomes. 2025 Jan 16;11(1):37-46. doi: 10.1093/ehjqcco/qcae014. Eur Heart J Qual Care Clin Outcomes. 2025. PMID: 38383606 Free PMC article.
-
Diabetes Life Expectancy Prediction Model Inputs and Results From Patient Surveys Compared With Electronic Health Record Abstraction: Survey Study.JMIR Aging. 2023 Nov 9;6:e44037. doi: 10.2196/44037. JMIR Aging. 2023. PMID: 37962566 Free PMC article.
-
What is the impact of multimorbidity on out-of-pocket healthcare expenditure among community-dwelling older adults in Ireland? A cross-sectional study.BMJ Open. 2022 Sep 1;12(9):e060502. doi: 10.1136/bmjopen-2021-060502. BMJ Open. 2022. PMID: 36581975 Free PMC article.
-
Association between adherence to antihypertensive medications and health outcomes in middle and older aged community dwelling adults; results from the Irish longitudinal study on ageing.Eur J Clin Pharmacol. 2019 Sep;75(9):1283-1292. doi: 10.1007/s00228-019-02699-w. Epub 2019 Jun 12. Eur J Clin Pharmacol. 2019. PMID: 31190134
-
Heterogeneity in Longitudinal Healthcare Utilisation by Older Adults: A Latent Transition Analysis of the Irish Longitudinal Study on Ageing.J Aging Health. 2022 Mar;34(2):253-265. doi: 10.1177/08982643211041818. Epub 2021 Sep 1. J Aging Health. 2022. PMID: 34470534 Free PMC article.
References
-
- Buurman BM, van den Berg W, Korevaar JC, Milisen K, de Haan RJ, de Rooij SE. Risk for poor outcomes in older patients discharged from an emergency department: feasibility of four screening instruments. European journal of emergency medicine: official journal of the European Society for Emergency Medicine. 2011;18(4):215–20. Epub 2011/02/15. 10.1097/MEJ.0b013e328344597e . - DOI - PubMed
-
- Short ME, Goetzel RZ, Pei X, Tabrizi MJ, Ozminkowski RJ, Gibson TB, et al. How accurate are self-reports? Analysis of self-reported health care utilization and absence when compared with administrative data. Journal of occupational and environmental medicine. 2009;51(7):786–96. Epub 2009/06/17. 10.1097/JOM.0b013e3181a86671 ; PubMed Central PMCID: PMCPmc2745402. - DOI - PMC - PubMed
-
- Reijneveld SA, Stronks K. The validity of self-reported use of health care across socioeconomic strata: a comparison of survey and registration data. Int J Epidemiol. 2001;30(6):1407–14. Epub 2002/02/01. . - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
