

Outcomes in dialysis versus conservative care for older patients: A prospective cohort analysis of stage 5 Chronic Kidney Disease
- PMID: 30365538
- PMCID: PMC6203391
- DOI: 10.1371/journal.pone.0206469
Outcomes in dialysis versus conservative care for older patients: A prospective cohort analysis of stage 5 Chronic Kidney Disease
Abstract
Background: The benefits of dialysis in older people with ESKD are not clear. We prospectively evaluated whether dialysis has survival advantage compared to conservative care (CC) in older people who were medically suitable for dialysis therapy.
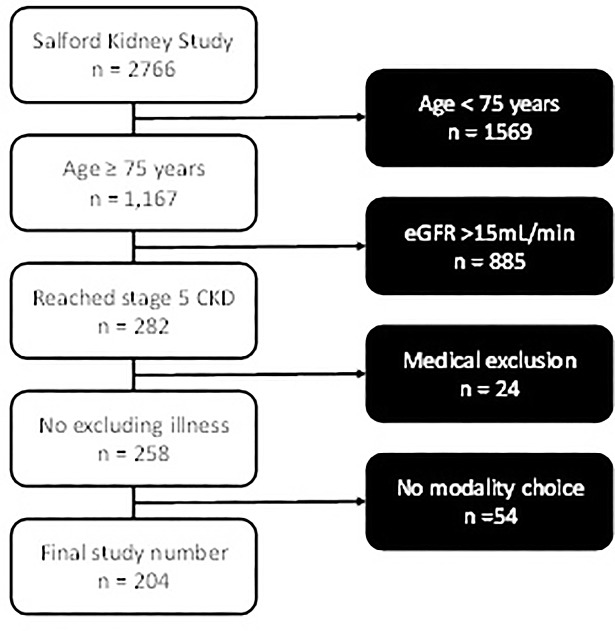
Methods: This was a prospective observational study of CKD patients aged ≥75 years when eGFR first reached ≤15ml/min/1.73m2. Hazard ratios (HR) for death were compared between patients who chose dialysis versus conservative care (CC) from when first seen in pre-dialysis clinic (eGFR ≤15ml/min/1.73m2), and when initiation of dialysis was first considered (eGFR ≤10ml/min/1.73m2). Patients with co-morbidities likely to significantly reduce life expectancy such as advanced heart failure, advanced dementia, and malignancy, were excluded.
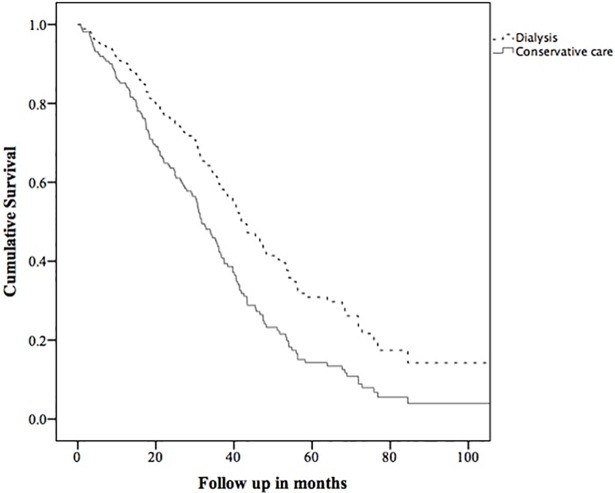
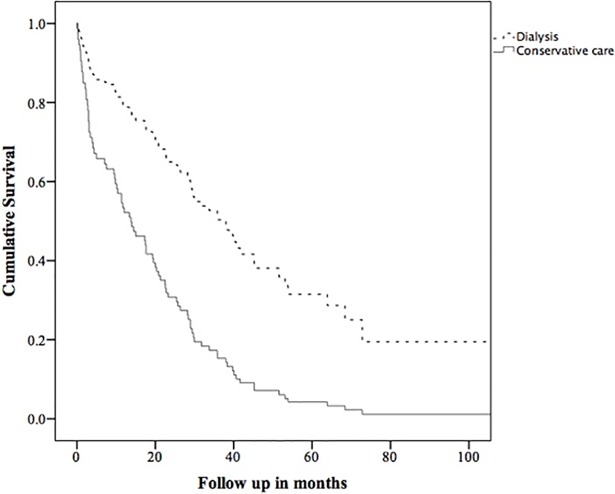
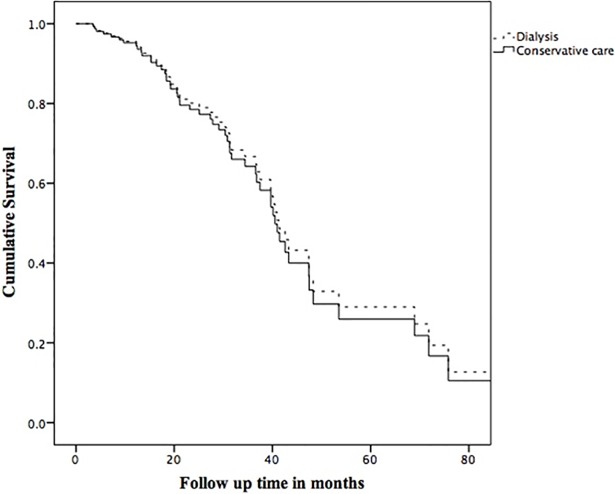
Results: There were 204 patients (123 dialysis, 81 CC). 115 went on to record eGFR of ≤10ml/min/1.73m2 (73 dialysis, 42 CC). The median survival from eGFR first ≤15ml/min/1.73m2 for the dialysis and CC groups were 42 (33-50) months and 31 (21-41) months. The adjusted hazard ratio (HR) for death in the dialysis group compared to CC was 0.61 (0.41-0.61, p = 0.01). The median survival from eGFR first ≤10ml/min/1.73m2 for dialysis and CC group were 36 (25-47) months and 12 (0-5) months. The adjusted HR for death in the dialysis group compared to CC was 0.36 (0.21-0.62, p <0.001).
Conclusion: Dialysis confers a survival benefit in older patients medically suitable for dialysis. This study is novel in being both prospective and in excluding patients with co-morbidities which may limit suitability for dialysis and life expectancy. A future focus on quality of life is needed to establish the true benefits of dialysis in older people.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Caskey F, Castledine C, Dawnay A, Farrington K, Fogarty D, Fraser S, et al. UK Renal Registry. 18th Annual Report of the Renal Association. Nephron. 2016; 132: 1–366.
-
- Lamping DL, Constantinovici N, Roderick P, Normand C, Henderson L, Harris S, et al. Clinical outcomes, quality of life, and costs in the North Thames Dialysis Study of elderly people on dialysis: a prospective cohort study. Lancet. 2000; 356(9241): 1543–1550. 10.1016/S0140-6736(00)03123-8 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
