

Integrating HIV care and treatment into tuberculosis clinics in Lusaka, Zambia: results from a before-after quasi-experimental study
- PMID: 30367622
- PMCID: PMC6204013
- DOI: 10.1186/s12879-018-3392-2
Integrating HIV care and treatment into tuberculosis clinics in Lusaka, Zambia: results from a before-after quasi-experimental study
Abstract
Background: Patients with HIV-associated tuberculosis (TB) often have their TB and HIV managed in separate vertical programs that offer care for each disease with little coordination. Such "siloed" approaches are associated with diagnostic and treatment delays, which contribute to unnecessary morbidity and mortality. To improve TB/HIV care coordination and early ART initiation, we integrated HIV care and treatment into two busy TB clinics in Zambia. We report here the effects of our intervention on outcomes of linkage to HIV care, early ART uptake, and TB treatment success for patients with HIV-associated TB in Lusaka, Zambia.
Methods: We provided integrated HIV treatment and care using a "one-stop shop" model intervention. All new or relapse HIV-positive TB patients were offered immediate HIV program enrolment and ART within 8 weeks of anti-TB therapy (ATT) initiation. We used a quasi-experimental design, review of routine program data, and survival analysis and logistic regression methods to estimate study outcomes before (June 1, 2010-January 31, 2011) and after (August 1, 2011-March 31, 2012) our intervention among 473 patients with HIV-associated TB categorized into pre- (n = 248) and post-intervention (n = 225) cohorts.
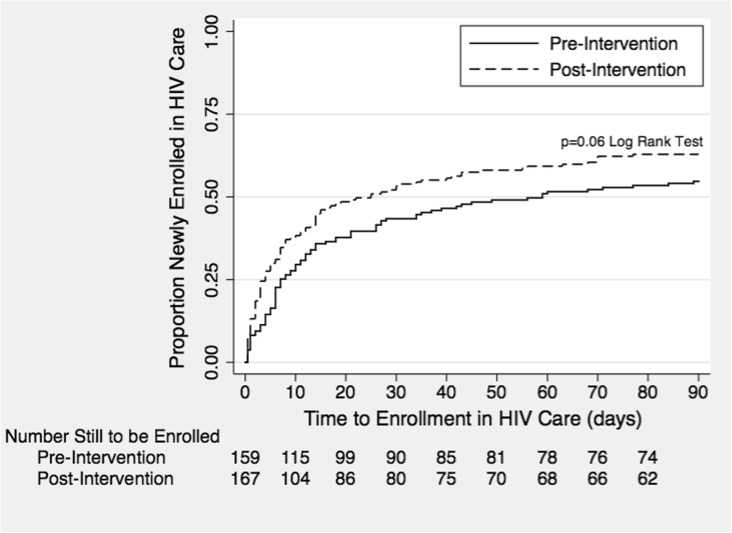
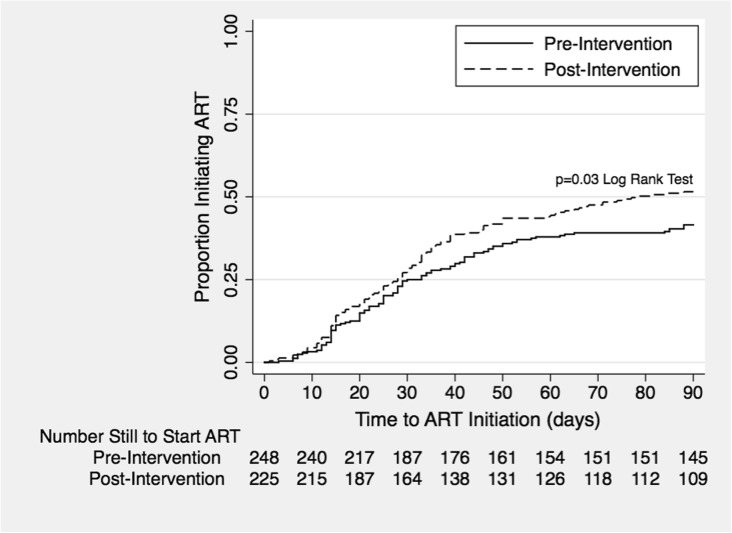
Results: Patients in the pre- and post-intervention cohorts were mostly male (60.1% and 52.9%, respectively) and young (median age: 33 years). In time-to-event analyses, a significantly higher proportion of patients in the post-intervention cohort linked to HIV care by 4 weeks post-ATT initiation (53.9% vs. 43.4%, p = 0.03), with median time to care linkage being 59 and 25 days in the pre- and post-intervention cohorts, respectively. In Cox proportional hazard modelling, patients receiving the integration intervention started ART by 8 weeks post-ATT at 1.33 times the rate (HR = 1.33, 95% CI: 1.00-1.77) as patients pre-intervention. In logistic regression modelling, patients receiving the intervention were 2.02 times (95% CI: 1.11-3.67) as likely to have a successful TB treatment outcome as patients not receiving the intervention.
Conclusions: Integrating HIV treatment and care services into routine TB clinics using a one-stop shop model increased linkage to HIV care, rates of early ART initiation, and TB treatment success among patients with HIV-associated TB in Lusaka, Zambia.
Keywords: Antiretroviral therapy; HIV/AIDS; Linkage to care; Sub-Saharan Africa; TB-HIV integration; Tuberculosis; Zambia.
Conflict of interest statement
Ethics approval and consent to participate
Ethical approval for this study was granted by the University of Zambia Biomedical Research Ethics Committee and the Institutional Review Board at the University of North Carolina at Chapel Hill, without requiring patient consent given the use of de-identified, routinely collected data.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- WHO . Global Tuberculosis Report. Geneva: World Health Organization; 2017. p. 249.
-
- Lawn SD, Campbell L, Kaplan R, Little F, Morrow C, Wood R. Ie DEASA: delays in starting antiretroviral therapy in patients with HIV-associated tuberculosis accessing non-integrated clinical services in a south African township. BMC Infect Dis. 2011;11:258. doi: 10.1186/1471-2334-11-258. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
