

Is there still a place for retroperitoneal lymph node dissection in clinical stage 1 nonseminomatous testicular germ-cell tumours? A retrospective clinical study
- PMID: 30367648
- PMCID: PMC6204050
- DOI: 10.1186/s12894-018-0412-x
Is there still a place for retroperitoneal lymph node dissection in clinical stage 1 nonseminomatous testicular germ-cell tumours? A retrospective clinical study
Abstract
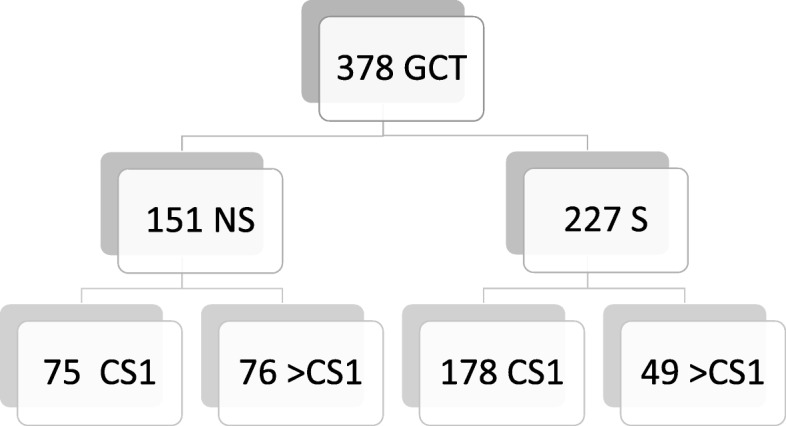
Background: Primary retroperitoneal lymph node dissection (RPLND) ultimately lost its role as the standard management of clinical stage (CS) 1 nonseminomatous (NS) testicular germ cell tumours (GCTs) in Europe when the European Germ Cell Cancer Consensus Group released their recommendations in 2008. Current guide-lines recommend surgery only for selected patients but reasons for selection remain rather ill-defined. We evaluated the practice patterns of the management of CS1 patients and looked specifically to the role of RPLND among other standard treatment options.
Methods: We retrospectively evaluated the treatment modalities of 75 consecutive patients treated for CS1 NS at one centre during 2008-2017. The patients undergoing RPLND were selected for a closer review. Particular reasons for surgery, clinical features of patients, and therapeutic outcome were analyzed using descriptive statistical methods.
Results: Twelve patients (16%) underwent nerve-sparing RPLND, nine surveillance, 54 had various regimens of adjuvant chemotherapy. Particular reasons for surgery involved illnesses precluding chemotherapy (n = 2), patients´ choice (n = 4), and teratomatous histology of the primary associated with equivocal radiologic findings (n = 6). Five patients had lymph node metastases, two received additional chemotherapy. Antegrade ejaculation was preserved in all cases. One patient had a grade 2 complication that was managed conservatively. All RPLND-patients remained disease-free.
Conclusions: Primary RPLND is a useful option in distinct CS1 patients, notably those with concurrent health problems precluding chemotherapy, and those with high proportions of teratoma in the primary associated with equivocal radiological findings. Informed patient's preference represents another acceptable reason for the procedure. RPLND properly suits the needs of well-selected patients with CS1 nonseminoma and deserves consideration upon clinical decision-making.
Keywords: Lymph node dissection; Nonseminomatous tumour; Teratoma; Testicular germ cell tumour.
Conflict of interest statement
Ethics approval and consent to participate
Ethical approval was provided by institutional ethical committee (Ethikkommission Albertinen-Krankenhaus Hamburg, ref. U3/2015 AKH). All patients consented to participate.
Consent for publication
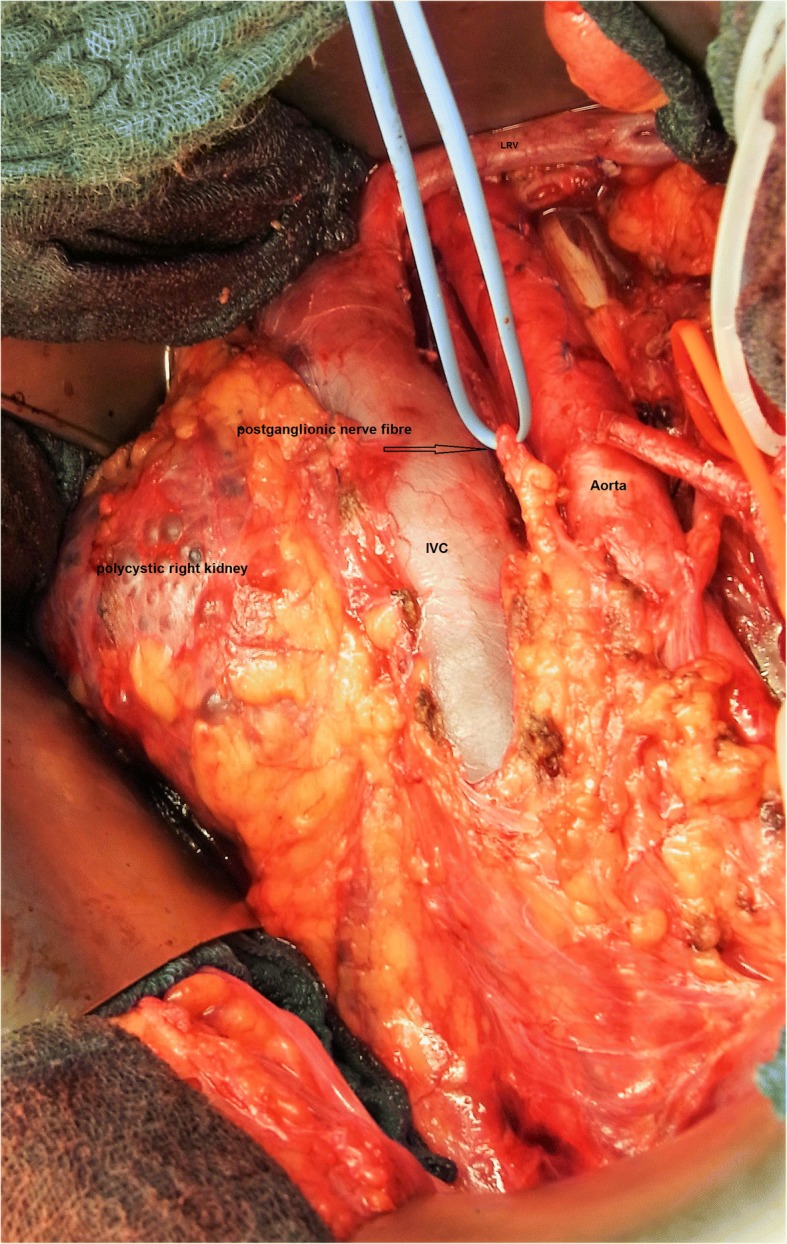
The patients relating to Figs. 2, 3, 4 and 5 gave written consent to publication of photographs showing details of their diseases. The documents are available from the corresponding author on reasonable request.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures



References
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
