

TRACE (Routine posTsuRgical Anesthesia visit to improve patient outComE): a prospective, multicenter, stepped-wedge, cluster-randomized interventional study
- PMID: 30367680
- PMCID: PMC6204052
- DOI: 10.1186/s13063-018-2952-5
TRACE (Routine posTsuRgical Anesthesia visit to improve patient outComE): a prospective, multicenter, stepped-wedge, cluster-randomized interventional study
Abstract
Background: Perioperative complications occur in 30-40% of non-cardiac surgical patients and are the leading cause of early postoperative morbidity and mortality. Regular visits by trained health professionals may decrease the incidence of complications and mortality through earlier detection and adequate treatment of complications. Until now, no studies have been performed on the impact of routine postsurgical anesthesia visits on the incidence of postoperative complications and mortality.
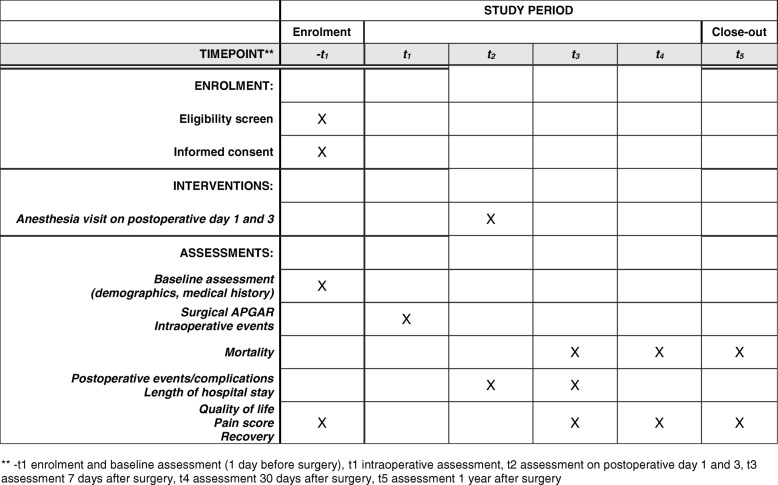
Methods: TRACE is a prospective, multicenter, stepped-wedge cluster randomized interventional study in academic and peripheral hospitals in the Netherlands. All hospitals start simultaneously with a control phase in which standard care is provided. Sequentially, in a randomized order, hospitals cross over to the intervention phase in which patients at risk are routinely followed up by an anesthesia professional at postoperative days 1 and 3, aiming to detect and prevent or treat postoperative complications. We aim to include 5600 adult patients who are at high risk of developing complications. The primary outcome variable is 30-day postoperative mortality. Secondary outcomes include incidence of postoperative complications and postoperative quality of life up to one year following surgery. Statistical analyses will be performed to compare the control and intervention cohorts with multilevel linear and logistic regression models, adjusted for temporal trends and for clusters (hospitals). The time horizon of the economic (cost-effectiveness) evaluation will be 30 days and one year following surgery.
Discussion: TRACE is the first to study the effects of a routine postoperative visit by an anesthesia healthcare professional on mortality and cost-effectiveness of surgical patients. If the intervention proves to be beneficial for the patient and cost-effective, the stepped-wedge design ensures direct implementation in the participating hospitals.
Trial registration: Nederlands Trial Register/Netherlands Trial Registration, NTR5506 . Registered on 02 December 2015.
Keywords: Anesthesiology; Failure-to-rescue; In-hospital mortality; Postsurgical complications; Stepped-wedge cluster randomized trial.
Conflict of interest statement
Ethics approval and consent to participate
Ethics approval is obtained from the institutional review board of the VUmc Amsterdam (NL56004.029.16; NTR5506). Patients will only be included in the study after written informed consent has been obtained.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

Similar articles
-
Routine Postsurgical Anesthesia Visit to Improve 30-day Morbidity and Mortality: A Multicenter, Stepped-wedge Cluster Randomized Interventional Study (The TRACE Study).Ann Surg. 2023 Mar 1;277(3):375-380. doi: 10.1097/SLA.0000000000004954. Epub 2021 May 24. Ann Surg. 2023. PMID: 34029230 Free PMC article. Clinical Trial.
-
The PRECious trial PREdiction of Complications, a step-up approach, CRP first followed by CT-scan imaging to ensure quality control after major abdominal surgery: study protocol for a stepped-wedge trial.Trials. 2015 Aug 28;16:382. doi: 10.1186/s13063-015-0903-y. Trials. 2015. PMID: 26314740 Free PMC article. Clinical Trial.
-
Influence of early goal-directed therapy using arterial waveform analysis on major complications after high-risk abdominal surgery: study protocol for a multicenter randomized controlled superiority trial.Trials. 2014 Sep 16;15:360. doi: 10.1186/1745-6215-15-360. Trials. 2014. PMID: 25227114 Free PMC article. Clinical Trial.
-
[Perioperative risk and mortality after major surgery].Anaesthesist. 2015 Nov;64(11):814-27. doi: 10.1007/s00101-015-0110-y. Anaesthesist. 2015. PMID: 26530399 Review. German.
-
Cost-Effectiveness Research in Anesthesiology.Anesth Analg. 2018 Nov;127(5):1196-1201. doi: 10.1213/ANE.0000000000003334. Anesth Analg. 2018. PMID: 29570150
Cited by
-
[Optimization of perioperative care of high-risk patients-a permanent challenge].Anaesthesist. 2019 Oct;68(10):651-652. doi: 10.1007/s00101-019-0627-6. Anaesthesist. 2019. PMID: 31637497 German. No abstract available.
-
Role of the anaesthetist in postoperative care.Br J Surg. 2020 Jan;107(2):e8-e10. doi: 10.1002/bjs.11395. Br J Surg. 2020. PMID: 31903603 Free PMC article.
-
The changing perspective of clinical trial designs.Perspect Clin Res. 2021 Apr-Jun;12(2):66-71. doi: 10.4103/picr.PICR_138_20. Epub 2021 Jan 8. Perspect Clin Res. 2021. PMID: 34012901 Free PMC article. Review.
-
Routine anaesthesia ward-based patient visits in surgery: 1-year outcomes of the TRACE randomized clinical trial.Br J Surg. 2025 Mar 4;112(3):znaf019. doi: 10.1093/bjs/znaf019. Br J Surg. 2025. PMID: 40071336 Free PMC article. Clinical Trial.
-
Routine Postsurgical Anesthesia Visit to Improve 30-day Morbidity and Mortality: A Multicenter, Stepped-wedge Cluster Randomized Interventional Study (The TRACE Study).Ann Surg. 2023 Mar 1;277(3):375-380. doi: 10.1097/SLA.0000000000004954. Epub 2021 May 24. Ann Surg. 2023. PMID: 34029230 Free PMC article. Clinical Trial.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
