

A 3-Dimensional Mapping Analysis of Regional Nodal Recurrences in Breast Cancer
- PMID: 30367906
- PMCID: PMC8135107
- DOI: 10.1016/j.ijrobp.2018.10.021
A 3-Dimensional Mapping Analysis of Regional Nodal Recurrences in Breast Cancer
Abstract
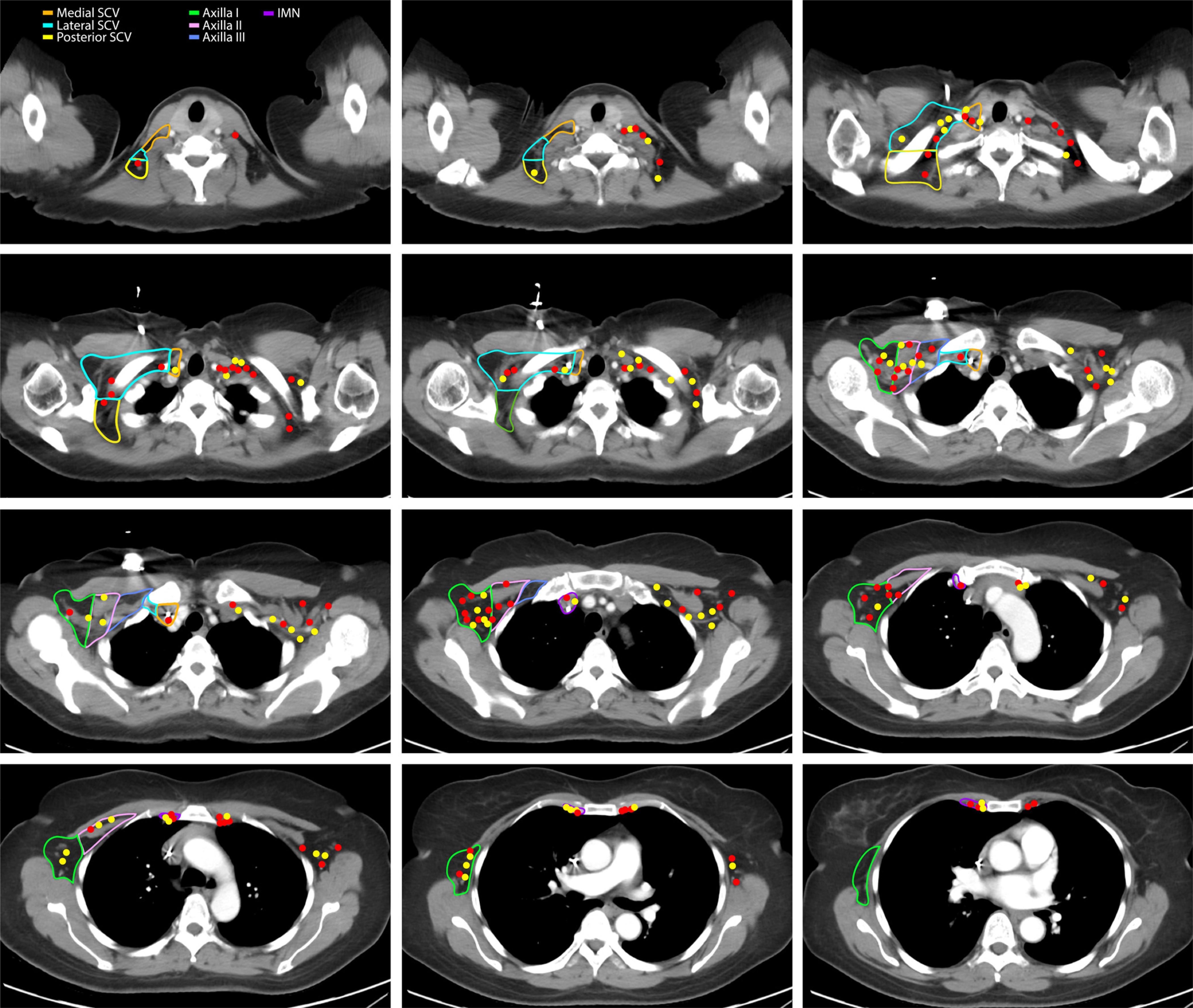
Purpose: The primary goal was to map the anatomic pattern of isolated nodal recurrences (NR) in the supraclavicular (SCV), axillary, and internal mammary nodes (IMNs) in patients with breast cancer treated with curative-intent surgery with or without radiation therapy (RT). Secondary objectives were to assess clinical and pathologic factors associated with patterns of NR and survival rates.
Methods and materials: Patients with NR after treatment at a single cancer center during 1998 to 2013 were identified. Patients with prior distant metastases or NR without correlative imaging were excluded. All NRs were overlaid onto representative axial computed tomographic images. Multivariable analysis was performed to identify clinical and pathologic characteristics associated with NR. Kaplan-Meier curves were generated to assess the rate of relapse by nodal region according to pathologic feature or radiation treatment status.
Results: The locations of 243 NRs among 153 eligible patients were mapped. The majority of NR occurred in the axilla (42%; 102/243), followed by the IMN (32.5%; 79/243) and the SCV (25.5%; 62/243). Radiation Therapy Oncology Group (RTOG) or European Society for Radiation therapy and Oncology (ESTRO) clinical target volume encompassed 82% (198/243) of NRs. The majority of out-of-field NRs were located in the lateral and posterior SCV region for both RTOG (67%; 30/45) and ESTRO (89%; 49/55) guidelines. The high-risk patients who received regional RT to the SCV relapsed at a similar rate in the medial, but a higher rate in lateral SCV (P = .009), compared with low-risk patients who received no nodal RT. Lymphovascular invasion most strongly associated with IMN NR (P = .001); grade 3 disease highly associated with both IMN (P = .001) and SCV NR (P = .02). The presence of an IMN NR portended for significantly inferior overall survival (OS), compared with an axillary NR, with a 5-year OS of 59% versus 72%, respectively (P = .03).
Conclusions: In this 3-dimensional image-based analysis of NR patterns in breast cancer patients treated with contemporary therapies, the lateral and posterior SCV represented a distinct site of NR that is not routinely included within current breast cancer contouring atlases. Grade 3 breast cancer and LVI were most commonly associated with the development of NR in the SCV. Modifying the CTV to encompass the lateral and posterior SCV in patients with breast cancer with these features might be justified.
Copyright © 2018 Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of interest: none.
Figures



Comment in
-
Image Guided Evolution of Nodal Contouring Guidelines in Breast Cancer.Int J Radiat Oncol Biol Phys. 2019 Mar 1;103(3):592-594. doi: 10.1016/j.ijrobp.2018.10.037. Int J Radiat Oncol Biol Phys. 2019. PMID: 30722970 No abstract available.
References
-
- Early Breast Cancer Trialists’ Collaborative G, Darby S, McGale P, Correa C, et al. Effect of radiotherapy after breast-conserving surgery on 10-year recurrence and 15-year breast cancer death: Meta-analysis of individual patient data for 10,801 women in 17 randomised trials. Lancet 2011;378:1707–1716. - PMC - PubMed
-
- Poortmans PM, Colette S, Kirkove C, et al. Internal mammary and medial supraclavicular irradiation in breast cancer. N Engl J Med 2015;373:317–327. - PubMed
-
- White J, Tai A, Arthur D, et al. RTOG breast cancer atlas; 2009. Available at: https://www.rtog.org/LinkClick.aspx?fileticket=vzJFhPaBipE%3d&tabid=236.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
