

Test-retest reliability of new and conventional echocardiographic parameters of left ventricular systolic function
- PMID: 30368567
- PMCID: PMC6426804
- DOI: 10.1007/s00392-018-1363-7
Test-retest reliability of new and conventional echocardiographic parameters of left ventricular systolic function
Abstract
Background: Reliability of left ventricular function measurements depends on actual biological conditions, repeated registrations and their analyses.
Objective: To investigate test-retest reliability of speckle-tracking-derived strain measurements and its determinants compared to the conventional parameters, such as ejection fraction (EF), LV volumes and mitral annular plane systolic excursion (MAPSE).
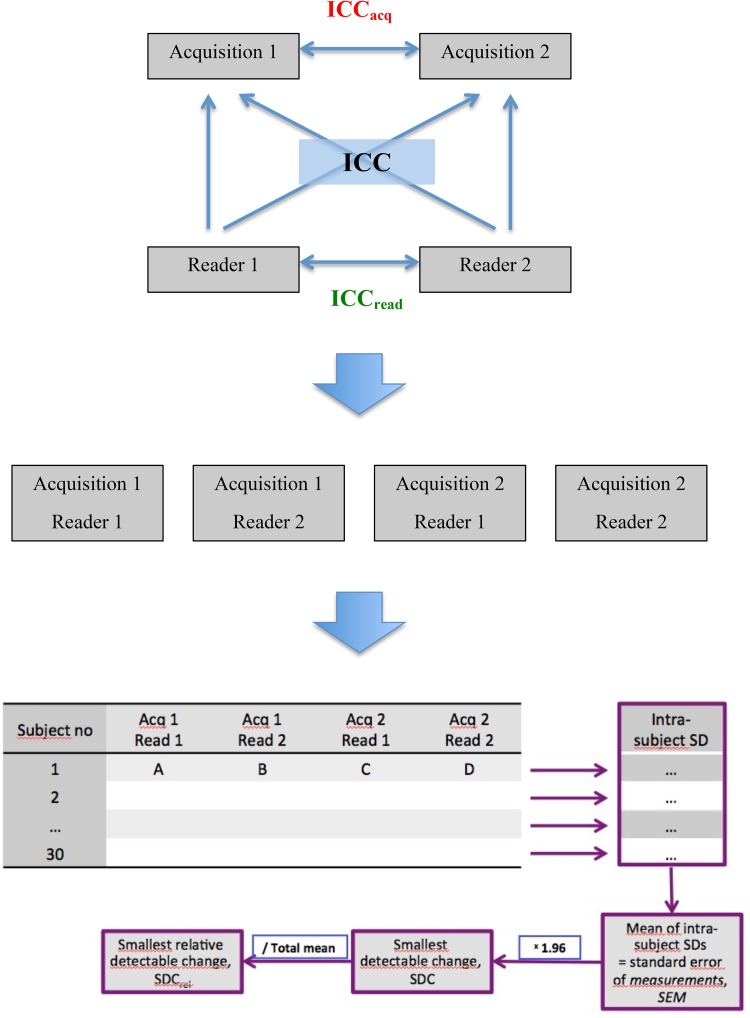
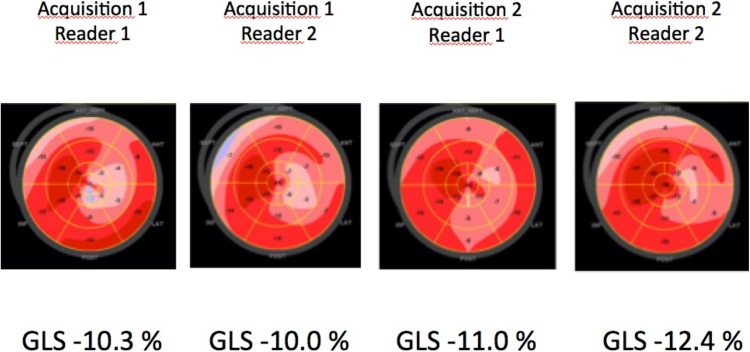
Methods: In 30 patients with a wide range of left ventricular function (mean EF 46.4 ± 16.4%, range 14-73%), standard echo views were acquired independently in a blinded fashion by two different echocardiographers in immediate sequence and analyzed off-line by two independent readers, creating 4 data sets per patient. Test-retest reliability of studied parameters was calculated using the smallest detectable change (SDC) and a total, inter-acquisition and inter-reader intra-class correlation coefficient (ICC).
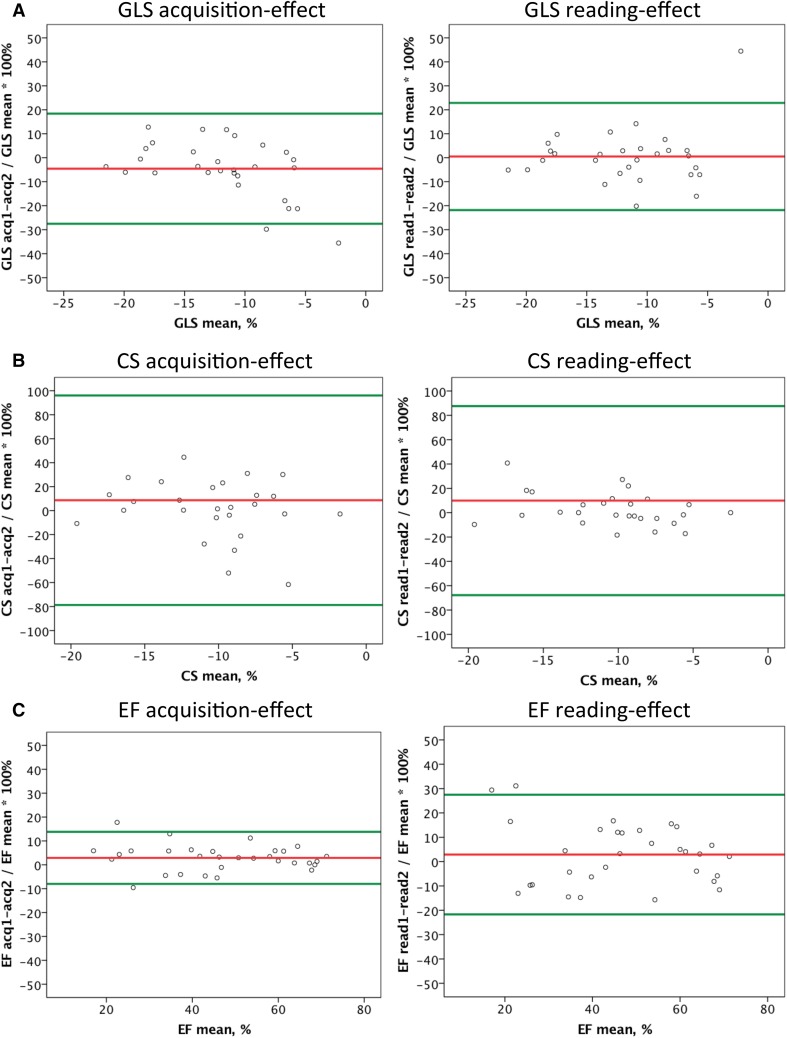
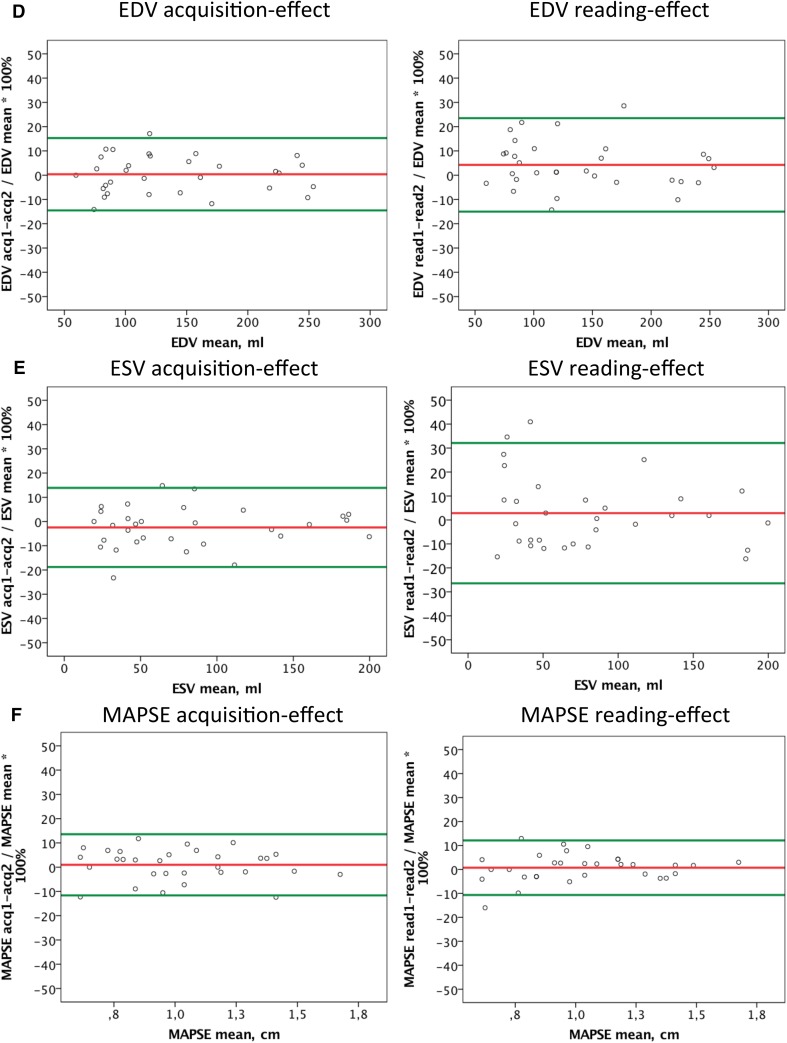
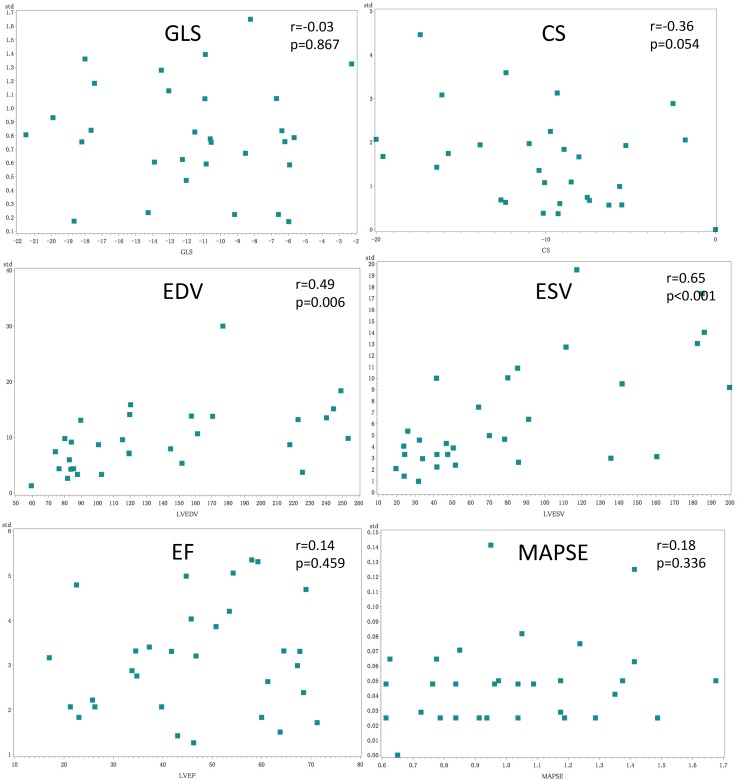
Results: The smallest detectable change normalized to the mean absolute value of the measured parameter (SDCrel) was lowest for MAPSE (10.7%). SDCrel for EF was similar to GLS (14.2 and 14.7%, respectively), while SDCrel for CS was much higher (35.6%). The intra-class correlation coefficient was excellent (> 0.9) for all measures of the left ventricular function. Intra-patient inter-acquisition reliability (ICCacq) was significantly better than inter-reader reliability (ICCread) (0.984 vs. 0.950, p = 0.03) only for EF, while no significant difference was observed for any other LV function parameter. Mean intra-subject standard deviations were significantly correlated to the mean values for CS and LV volumes, but not for the other studied parameters.
Conclusions: In a test-retest setting, both with normal and impaired left ventricular function, the smallest relative detectable change of EF, GLS and MAPSE was similar (11-15%), but was much higher for CS (35%). Surprisingly, reliability of GLS was not superior to that of EF. Acquisition and reader to a similar extent influenced the reliability of measurements of all left ventricular function measures except for ejection fraction, where the reliability was more dependent on the reader than on the acquisition.
Keywords: Ejection fraction; Global longitudinal strain; Left ventricular function; Mitral annulus plane systolic excursion; Test–retest reliability.
Conflict of interest statement
The author declares that there is no competing interest.
Figures
References
-
- Barbier P, Mirea O, Cefalù C, Maltagliati A, Savioli G, Guglielmo M. Reliability and feasibility of longitudinal AFI global and segmental strain compared with 2D left ventricular volumes and ejection fraction: intra- and inter-operator, test–retest, and inter-cycle reproducibility. Eur Heart J Cardiovasc Imaging. 2015;16:642–652. doi: 10.1093/ehjci/jeu274. - DOI - PubMed
-
- Huttin O, Marie PY, Benichou M, Bozec E, Lemoine S, Mandry D, et al. Temporal deformation pattern in acute and late phases of ST-elevation myocardial infarction: incremental value of longitudinal post-systolic strain to assess myocardial viability. Clin Res Cardiol. 2016;105:815–826. doi: 10.1007/s00392-016-0989-6. - DOI - PubMed
-
- Tschöpe C, Birner C, Böhm M, Bruder O, Frantz S, Luchner A, et al. Heart failure with preserved ejection fraction: current management and future strategies: expert opinion on the behalf of the Nucleus of the “Heart Failure Working Group” of the German Society of Cardiology (DKG) Clin Res Cardiol. 2018;107:1–19. doi: 10.1007/s00392-017-1170-6. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
