

[Efficacy and safety of decitabine in combination with G-CSF, low-dose cytarabine and aclarubicin in MDS-EB and AML-MRC]
- PMID: 30369183
- PMCID: PMC7342258
- DOI: 10.3760/cma.j.issn.0253-2727.2018.09.006
[Efficacy and safety of decitabine in combination with G-CSF, low-dose cytarabine and aclarubicin in MDS-EB and AML-MRC]
Abstract
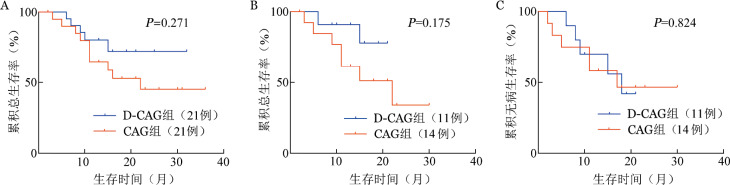
Objective: To evaluate the clinical efficacy and safety of decitabine in combination with lower-dose CAG regimen (G-CSF, cytarabine and aclarubicin; D-CAG regimen) in the treatment of myelodysplastic syndromes with excess blasts (MDS-EB) and acute myeloid leukemia with myelodysplasia-related changes (AML-MRC), compared to standard CAG regimen. Methods: A total of 42 patients with newly diagnosed MDS-EB and AML-MRC from May 2011 to March 2017 were included in the retrospective study. 21 cases were initially treated with G-CSF for priming, in combination with cytarabine of 10 mg/m(2) q12h for 14 days and aclarubicin of 20 mg/d for 4 days (CAG regimen) and the other 21 cases were initially treated with decitabine of 20 mg/m(2) for 5 days and lower-dose CAG regimen (cytarabine of 10 mg/m(2) q12h for 7 days, aclarubicin of 10 mg/d for 4 days, and G-CSF for priming (D-CAG regimen). After two cycles of induction chemotherapy, the patients who obtained complete remission(CR) received consolidation chemotherapy or hematopoietic stem cell transplantation (HSCT). Results: Among a total of 42 patients, the median age was 52.5 years (18-65 years) and 64.3% of them were male. Baseline characteristics of patients between D-CAG group and CAG group showed no significant differences. The CR for patients in D-CAG group was 81.0% (17/21), compared to 52.4% (11/21) in CAG group after 2 cycles of therapy (χ(2)=3.857, P=0.050). The overall response rate (ORR) for patients in D-CAG group and CAG group was 85.7% (18/21) and 76.2% (15/21) respectively, without significant difference (χ(2)=1.273, P=0.259). By December 2017, the median follow-up of D-CAG group and CAG group was 13(6-32) months and 15(2-36) months respectively. Finally, 10 patients in D-CAG group and 7 patients in CAG group received HSCT respectively. Except patients receiving HSCT, the median leukemia-free survival (LFS) time for patients in D-CAG group and CAG group was 18.0 (95%CI 6.6-29.4) months and 11.0 (95%CI 0-23.9) months respectively. Probabilities of 12 months LFS for D-CAG group and CAG group were (63.6±14.5)% and (50.0±13.4)% respectively, without difference (χ(2)=0.049, P=0.824). Except patients receiving HSCT, there were 2 deaths in D-CAG group and 7 deaths in CAG group respectively. The cumulative probabilities of 12 months OS for non-HSCT patients in D-CAG group and CAG group were (90.9±8.7)% and (61.5±13.5)% respectively, without significant difference (χ(2)=1.840, P=0.175). The incidences of side effects between D-CAG group and CAG group did not show significant differences (P=0.479), and the main side effects included cytopenias, pneumonia, infections of skin and soft tissues, neutropenic patients with fever, liver dysfunction. Conclusion: The decitabine in combination with lower-dose CAG regimen improved CR for patients with MDS-EB and AML-MRC, and was a promising choice.
目的: 比较地西他滨(DAC)联合半量CAG方案(D-CAG)与CAG方案治疗骨髓增生异常综合征伴原始细胞增多(MDS-EB)和急性髓系白血病伴骨髓增生异常相关改变(AML-MRC)的临床疗效及安全性。 方法: 回顾性分析2011年5月至2017年3月42例初治MDS-EB和AML-MRC患者临床资料,21例接受D-CAG治疗,21例接受CAG方案治疗,诱导缓解后患者继续巩固化疗或进行allo-HSCT。比较两组患者的CR率、总有效率(ORR)、总生存(OS)率、无病生存(DFS)率和不良反应发生率。 结果: 42例MDS-EB和AML-MRC患者中,男27例,女15例,中位年龄52.5(18~65)岁;MDS-EB 21例,AML-MRC 21例。D-CAG组和CAG组年龄、性别、疾病类型、基因突变类型和染色体核型差异均无统计学意义。D-CAG组2个疗程CR率为81.0%(17/21),高于CAG组的52.4%(11/21)(χ(2)=3.857,P=0.050)。D-CAG组与CAG组2个疗程后ORR分别为85.7%(18/21)与76.2%(15/21),差异无统计学意义(χ(2)=1.273,P=0.259)。D-CAG组和CAG组的中位随访时间分别为13(6~32)个月和15(2~36)个月,D-CAG组10例患者接受了allo-HSCT,CAG组7例患者接受了allo-HSCT。D-CAG组非移植患者的中位LFS时间为18.0(95%CI 6.6~29.4)个月,CAG组非移植患者的中位LFS时间为11.0(95%CI 0~23.9)个月,两组1年累积LFS率分别为(63.6±14.5)%和(50.0±13.4)%,差异无统计学意义(χ(2)=0.049,P=0.824)。D-CAG组11例非移植患者中2例死亡,CAG组非移植的14例患者中7例死亡,D-CAG组与CAG组非移植患者的1年累积OS率为(90.9±8.7)%对(61.5±13.5)%,D-CAG组高于CAG组,但差异无统计学意义(χ(2)=1.840,P=0.175)。D-CAG组主要的不良反应为骨髓抑制所致的感染,化疗后肺部感染发生率为42.9%,与CAG组(38.1%)差异无统计学意义(P=0.753)。 结论: DAC联合半量CAG方案治疗初治MDS-EB和AML-MRC患者的CR率高于CAG方案,且不良反应与CAG方案相当,对患者长期生存的影响有待进一步观察。.
Keywords: CAG regimen; D-CAG regimen; Myelodysplastic syndromes; Treatment outcome.
Figures
Similar articles
-
[The clinical efficacy of the patients of acute myeloid leukemia and myelodysplastic syndromes treated with decitabine alone, combined with half or one couse of CAG regimen].Zhonghua Xue Ye Xue Za Zhi. 2014 Nov;35(11):961-5. doi: 10.3760/cma.j.issn.0253-2727.2014.11.001. Zhonghua Xue Ye Xue Za Zhi. 2014. PMID: 25417868 Chinese.
-
Decitabine in the Treatment of Acute Myeloid Leukemia and Myelodysplastic Syndromes, Which Combined with Complex Karyotype Respectively.Asian Pac J Cancer Prev. 2015;16(15):6627-32. doi: 10.7314/apjcp.2015.16.15.6627. Asian Pac J Cancer Prev. 2015. PMID: 26434886
-
Cladribine with Granulocyte Colony-Stimulating Factor, Cytarabine, and Aclarubicin Regimen in Refractory/Relapsed Acute Myeloid Leukemia: A Phase II Multicenter Study.Oncologist. 2020 Nov;25(11):e1663-e1670. doi: 10.1634/theoncologist.2020-0818. Epub 2020 Sep 21. Oncologist. 2020. PMID: 32845551 Free PMC article. Clinical Trial.
-
A meta-analysis of CAG (cytarabine, aclarubicin, G-CSF) regimen for the treatment of 1029 patients with acute myeloid leukemia and myelodysplastic syndrome.J Hematol Oncol. 2011 Nov 14;4:46. doi: 10.1186/1756-8722-4-46. J Hematol Oncol. 2011. PMID: 22082134 Free PMC article. Review.
-
D-CAG (decitabine followed by cytarabine, aclarubicin, and G-CSF) for relapsed acute myeloid leukemia after hematopoietic cell transplantation.Ann Hematol. 2016 Jan;95(1):157-159. doi: 10.1007/s00277-015-2505-x. Epub 2015 Sep 18. Ann Hematol. 2016. PMID: 26382274 Review. No abstract available.
Cited by
-
Patients with AML-MRC benefit from decitabine in combination with low-dose G-CSF, cytarabine and aclarubicin: A single center cohort study.Leuk Res Rep. 2022 Oct 19;18:100354. doi: 10.1016/j.lrr.2022.100354. eCollection 2022. Leuk Res Rep. 2022. PMID: 36304522 Free PMC article.
-
Dual Growth Factor (rhTPO + G-CSF) and Chemotherapy Combination Regimen for Elderly Patients with Acute Myeloid Leukemia: A Phase II Single-Arm Multicenter Study.Int J Gen Med. 2021 Sep 27;14:6093-6099. doi: 10.2147/IJGM.S323699. eCollection 2021. Int J Gen Med. 2021. PMID: 34611424 Free PMC article. Clinical Trial.
-
Decitabine-containing G-CSF priming regimen overcomes resistance of primary mediastinal neoplasm from early T-cell precursors to conventional chemotherapy: a case report.Onco Targets Ther. 2019 Aug 29;12:7039-7044. doi: 10.2147/OTT.S214905. eCollection 2019. Onco Targets Ther. 2019. PMID: 31507324 Free PMC article.
-
Homoharringtonine combined with cladribine and aclarubicin (HCA) in acute myeloid leukemia: A new regimen of conventional drugs and its mechanism.Oxid Med Cell Longev. 2022 Jul 13;2022:8212286. doi: 10.1155/2022/8212286. eCollection 2022. Oxid Med Cell Longev. 2022. PMID: 35873796 Free PMC article.
References
-
- 王 萍. 超小剂量的地西他滨联合CAG方案治疗中高危骨髓增生异常综合征及难治性白血病的效果分析[J] 中国继续医学教育. 2016;8(5):146–147.
-
- 乔 爱国. 地西他滨联合小剂量CAG方案治疗骨髓增生异常综合征疗效观察[J] 世界最新医学信息文摘(连续型电子期刊) 2015;15(98):20–21.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous