

Determinants of Long-Term Outcomes and Costs in the Management of Critical Limb Ischemia: A Population-Based Cohort Study
- PMID: 30369325
- PMCID: PMC6201392
- DOI: 10.1161/JAHA.118.009724
Determinants of Long-Term Outcomes and Costs in the Management of Critical Limb Ischemia: A Population-Based Cohort Study
Abstract
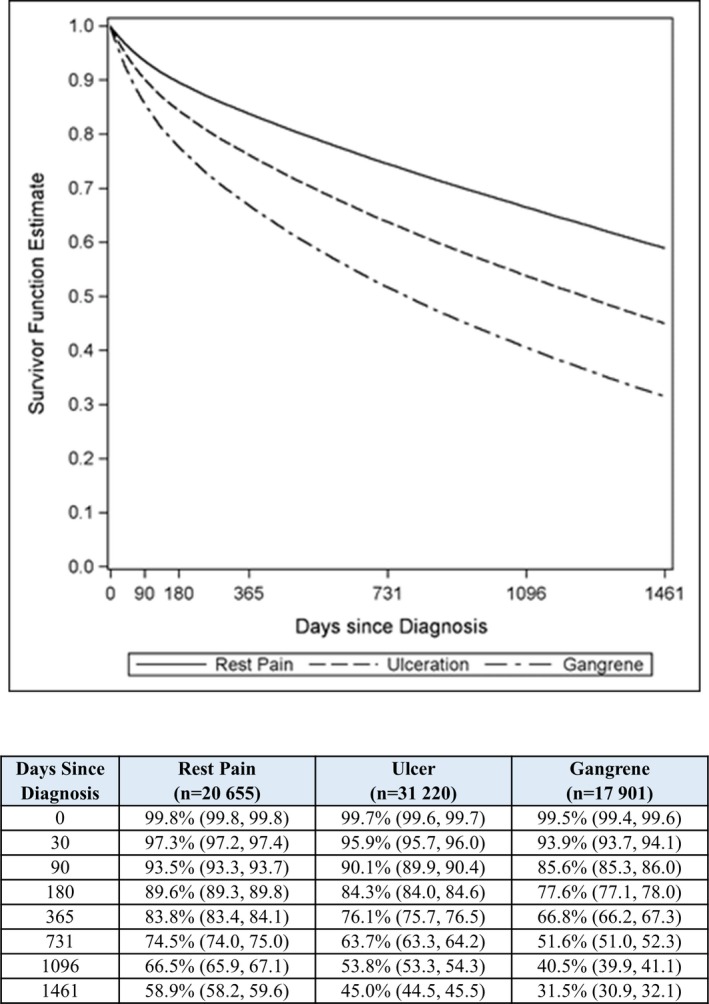
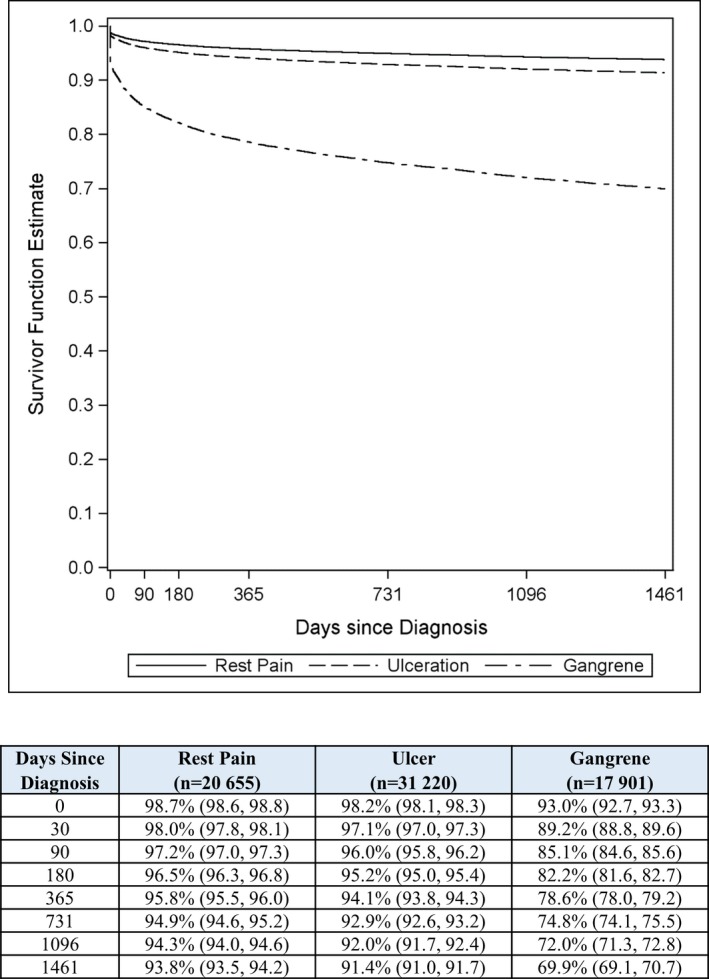
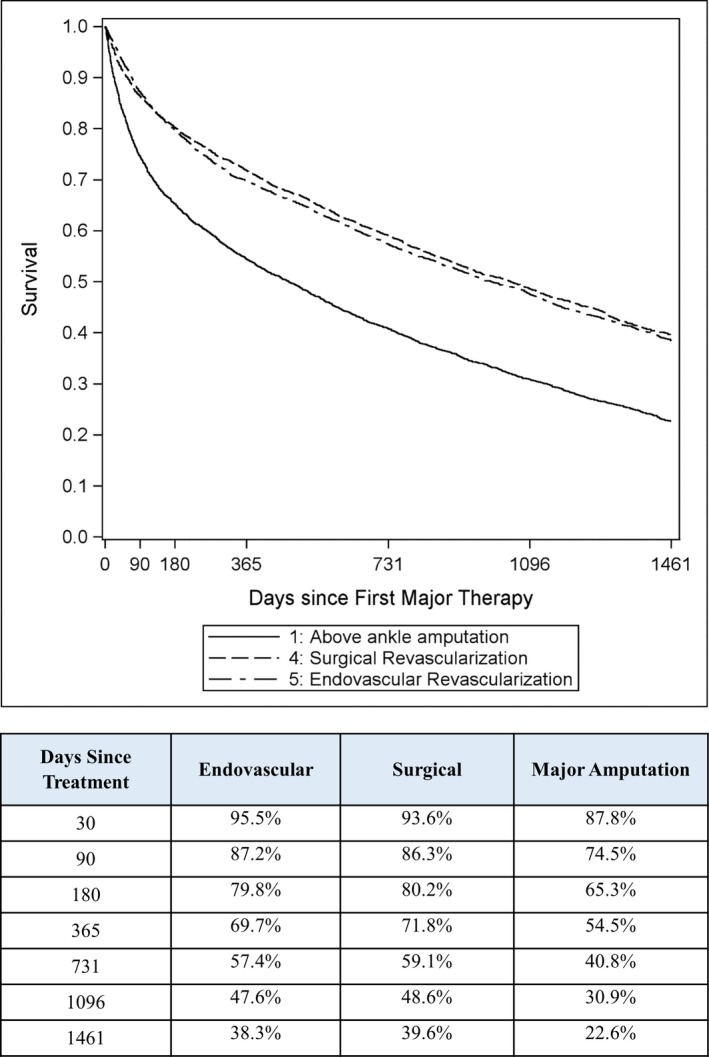
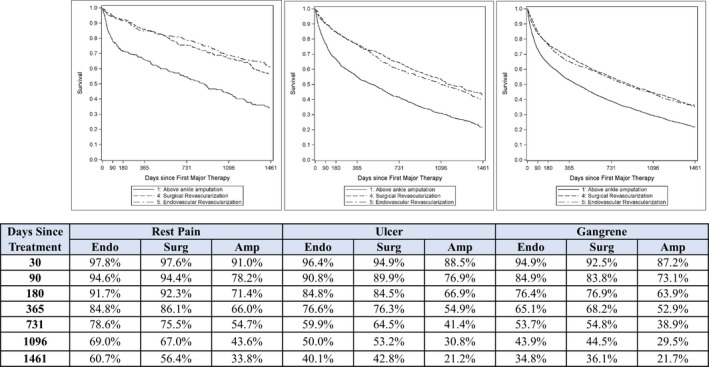
Background The optimal treatment for critical limb ischemia remains controversial owing to conflicting conclusions from previous studies. Methods and Results We obtained administrative claims on Medicare beneficiaries with initial critical limb ischemia diagnosis in 2011. Clinical outcomes and healthcare costs over 4 years were estimated among all patients and by first treatment (endovascular revascularization, surgical revascularization, or major amputation) in unmatched and propensity-score-matched samples. Among 72 199 patients with initial primary critical limb ischemia diagnosis in 2011, survival was 46% (median survival, 3.5 years) and freedom from major amputation was 87%. Among 9942 propensity-score-matched patients (8% rest pain, 26% ulcer, and 66% gangrene), survival was 38% with endovascular revascularization (median survival, 2.7 years), 40% with surgical revascularization (median survival, 2.9 years), and 23% with major amputation (median survival, 1.3 years; P<0.001 for each revascularization procedure versus major amputation). Corresponding major amputation rates were 6.5%, 9.6%, and 10.6%, respectively ( P<0.001 for all pair-wise comparisons). The cost per patient year during follow-up was $49 700, $49 200, and $55 700, respectively ( P<0.001 for each revascularization procedure versus major amputation). Conclusions Long-term survival and cost in critical limb ischemia management is comparable between revascularization techniques, with lower major amputation rates following endovascular revascularization. Primary major amputation results in shorter survival, higher risk of subsequent major amputation, and higher healthcare costs versus revascularization. Results from this observational research may be susceptible to bias because of the influence of unmeasured confounders.
Keywords: Medicare; amputation; cost; critical limb ischemia; peripheral artery disease; revascularization.
Figures
Comment in
-
Worth an Arm and a Leg: The Critical Importance of Limb Ischemia.J Am Heart Assoc. 2018 Aug 21;7(16):e010093. doi: 10.1161/JAHA.118.010093. J Am Heart Assoc. 2018. PMID: 30369333 Free PMC article. No abstract available.
References
-
- Gerhard‐Herman MD, Gornik HL, Barrett C, Barshes NR, Corriere MA, Drachman DE, Fleisher LA, Fowkes FG, Hamburg NM, Kinlay S, Lookstein R, Misra S, Mureebe L, Olin JW, Patel RA, Regensteiner JG, Schanzer A, Shishehbor MH, Stewart KJ, Treat‐Jacobson D, Walsh ME. 2016 AHA/ACC Guideline on the management of patients with lower extremity peripheral artery disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2017;69:e71–e126. - PubMed
-
- Siracuse JJ, Menard MT, Eslami MH, Kalish JA, Robinson WP, Eberhardt RT, Hamburg NM, Farber A; Vascular Quality Initiative . Comparison of open and endovascular treatment of patients with critical limb ischemia in the Vascular Quality Initiative. J Vasc Surg. 2016;63:958–965.e1. - PubMed
-
- Bisdas T, Borowski M, Stavroulakis K, Torsello G; CRITISCH Collaborators . Endovascular therapy versus bypass surgery as first‐line treatment strategies for critical limb ischemia: results of the interim analysis of the CRITISCH Registry. JACC Cardiovasc Interv. 2016;9:2557–2565. - PubMed
-
- Adam DJ, Beard JD, Cleveland T, Bell J, Bradbury AW, Forbes JF, Fowkes FG, Gillepsie I, Ruckley CV, Raab G, Storkey H; BASIL trial participants . Bypass versus angioplasty in severe ischaemia of the leg (BASIL): multicentre, randomised controlled trial. Lancet. 2005;366:1925–1934. - PubMed
-
- Armstrong EJ, Ryan MP, Baker ER, Martinsen BJ, Kotlarz H, Gunnarsson C. Risk of major amputation or death among patients with critical limb ischemia initially treated with endovascular intervention, surgical bypass, minor amputation, or conservative management. J Med Econ. 2017;20:1148–1154. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
