

Epidemiological and imaging features that can affect the detection of ureterolithiasis on ultrasound
- PMID: 30369654
- PMCID: PMC6198834
- DOI: 10.1590/0100-3984.2017.0113
Epidemiological and imaging features that can affect the detection of ureterolithiasis on ultrasound
Abstract
Objective: To identify, in patients with clinical suspicion of ureterolithiasis, epidemiological and imaging features that affect calculus detection on ultrasound, as well as to compare ultrasound with multidetector computed tomography (MDCT).
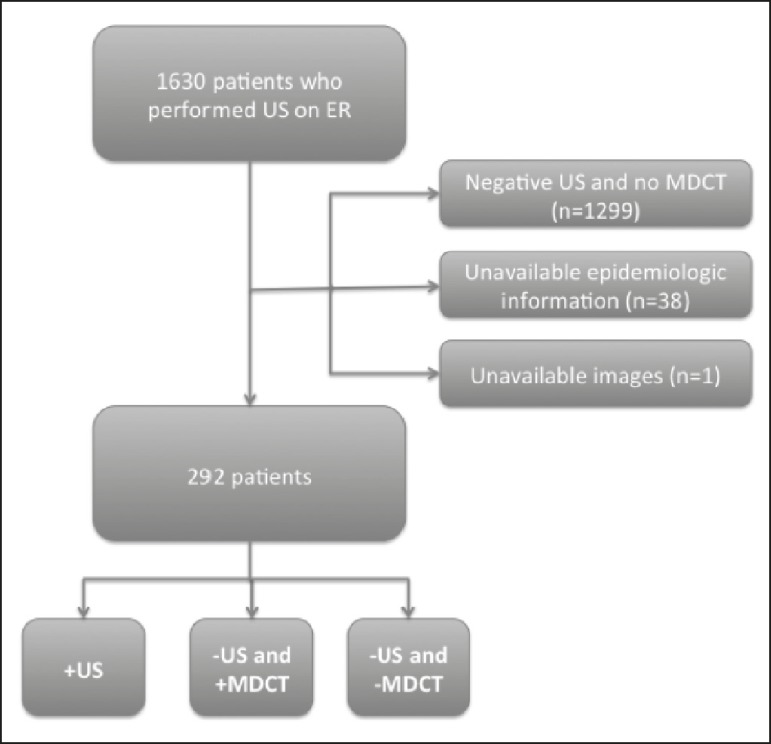
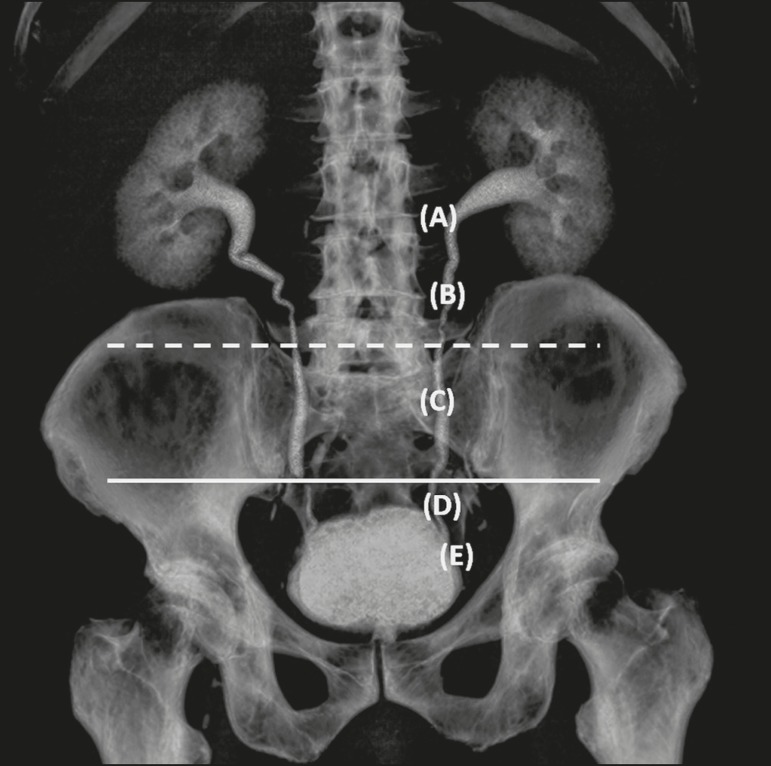
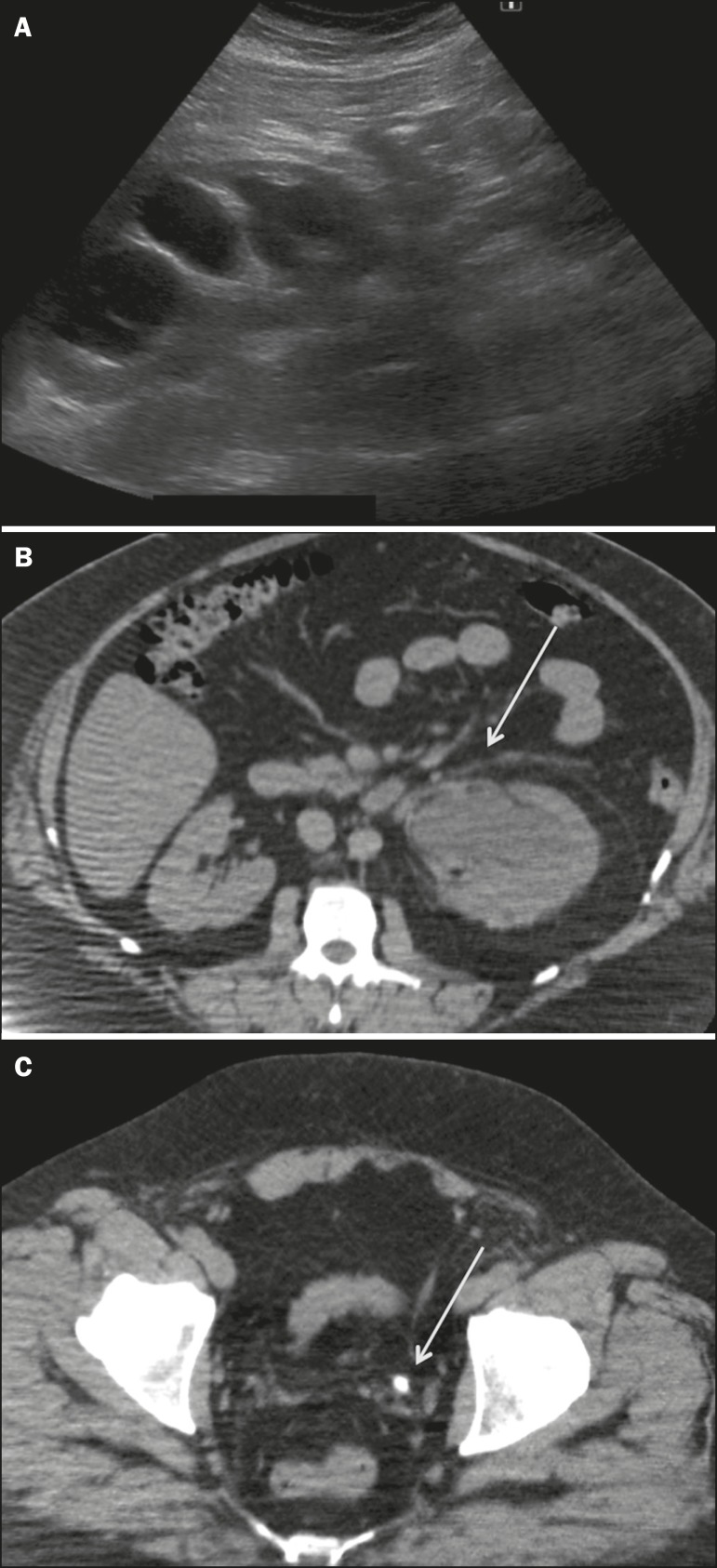
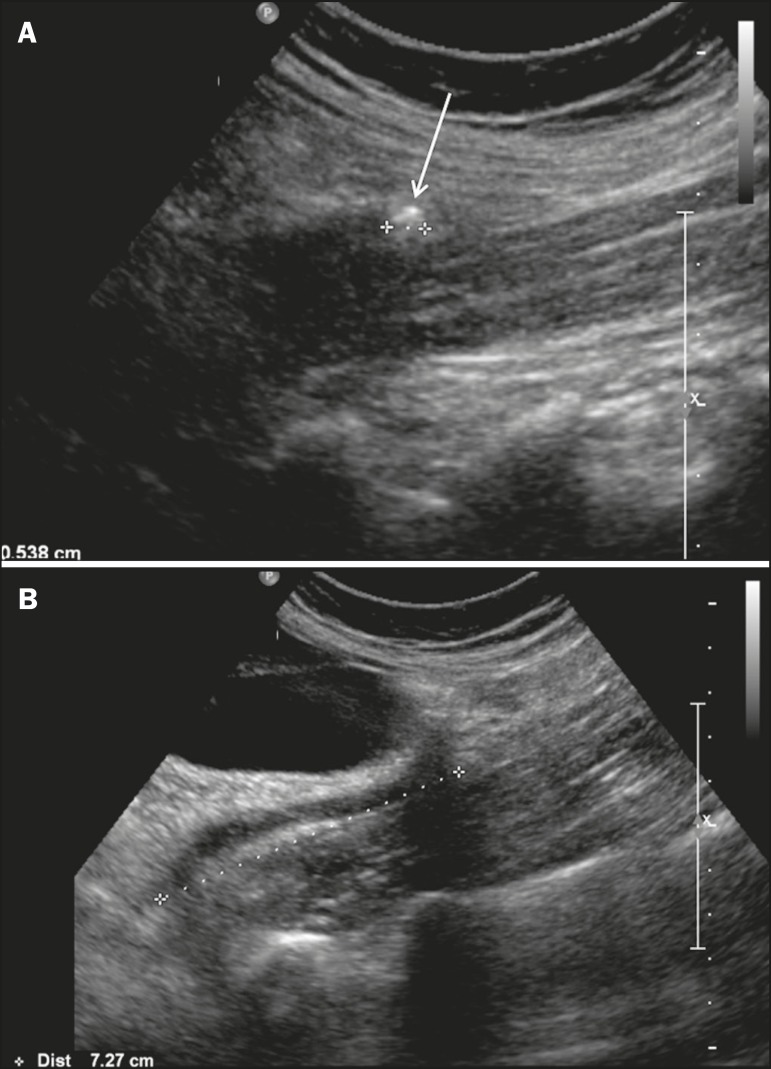
Materials and methods: We searched our database for patients who underwent ultrasound, followed by MDCT (if the ultrasound was negative), for suspected ureterolithiasis in an emergency setting. Patients were divided into three groups: positive ultrasound (US+); negative ultrasound/positive MDCT (US-/MDCT+); and negative ultrasound/negative MDCT (US-/MDCT-). We evaluated age, gender, ureterolithiasis laterality, location of the calculus within the ureter, body mass index, calculus diameter, and calculus attenuation on MDCT.
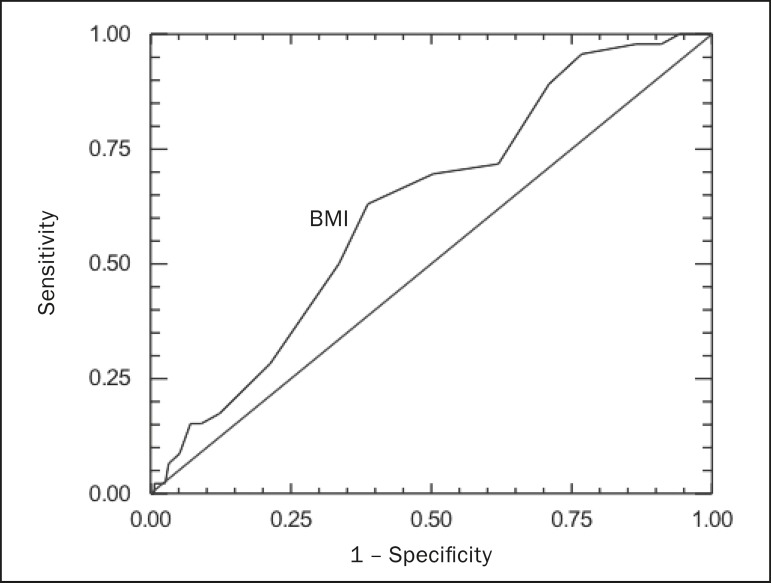
Results: Of a total of 292 cases of suspected ureterolithiasis, 155 (53.1%) were in the US+ group, 46 (15.7%) were in the US-/MDCT+ group, and 91 (31.2%) were in the US-/MDCT- group. There were no significant differences among the groups in terms of age, gender, ureterolithiasis laterality, and mean MDCT attenuation values. Distal ureterolithiasis was most common in the US+ group, and calculi at other ureteral locations were more common in the US-/MDCT+ group. The mean body mass index was significantly higher in the US-/MDCT+ group than in the US+ group, and the mean calculus diameter was significantly greater in the US+ group than in the US-/MDCT+ group.
Conclusion: A high body mass index, large calculus diameter, and calculus location in the distal third of the ureter are the major factors favoring ureterolithiasis detection on ultrasound.
Objetivo: Identificar achados epidemiológicos e de imagem em pacientes com suspeita clínica de ureterolitíase que afetam a detecção do cálculo no ultrassom (US), comparado com a tomografia computadorizada multidetectores (TCMD).
Materiais e métodos: Procuramos, em nosso banco de dados, por pacientes que realizaram US no serviço de emergência, seguido por TCMD (se US negativo), por suspeita de ureterolitíase. Os pacientes foram divididos em: 1) US positivo; 2) US negativo e TCMD positiva; 3) US e TCMD negativos. Avaliamos idade, sexo, lateralidade, localização ureteral, índice de massa corporal, diâmetro e densidade do cálculo.
Resultados: Foram incluídos no estudo 292 pacientes. Constatamos que 53,1% das ureterolitíases foram detectadas por US (grupo 1), 15,7% apenas por TCMD (grupo 2), e em 31,2% ambos os métodos foram negativos (grupo 3). Idade, sexo, lateralidade e densidade do cálculo pela TCMD não tiveram diferença significativa entre os grupos. No grupo 1, ureterolitíase foi detectada, preferencialmente, em localização distal, e fora do ureter distal no grupo 2. O índice de massa corporal foi significativamente maior em pacientes do grupo 2, comparado ao grupo 1. O diâmetro do cálculo detectado no grupo 1 foi significativamente maior do que no grupo 2.
Conclusão: Índice de massa corporal, diâmetro e localização do cálculo no terço distal do ureter foram os principais fatores que contribuíram para a detecção do cálculo pelo US.
Keywords: Body mass index; Tomography, X-ray computed; Ultrasonography; Ureterolithiasis.
Figures
Similar articles
-
Unenhanced helical CT of ureterolithiasis: value of the tissue rim sign.AJR Am J Roentgenol. 1997 Apr;168(4):997-1000. doi: 10.2214/ajr.168.4.9124157. AJR Am J Roentgenol. 1997. PMID: 9124157
-
The sensitivity of transabdominal ultrasound in the diagnosis of ureterolithiasis.Med Ultrason. 2010 Sep;12(3):188-97. Med Ultrason. 2010. PMID: 21203595
-
Cost-effectiveness analysis (CEA) of intravenous urography (IVU) and unenhanced multidetector computed tomography (MDCT) for initial investigation of suspected acute ureterolithiasis.Acta Radiol. 2008 Mar;49(2):222-9. doi: 10.1080/02841850701708304. Acta Radiol. 2008. PMID: 18300151 Clinical Trial.
-
Conventional and reduced radiation dose of 16-MDCT for detection of nephrolithiasis and ureterolithiasis.AJR Am J Roentgenol. 2008 Jan;190(1):151-7. doi: 10.2214/AJR.07.2816. AJR Am J Roentgenol. 2008. PMID: 18094305
-
Limited sensitivity and size over measurements of ultrasound affect medical decisions for ureteral stone compared to non-contrasted computed tomography.World J Urol. 2019 May;37(5):907-911. doi: 10.1007/s00345-018-2444-y. Epub 2018 Aug 14. World J Urol. 2019. PMID: 30109485
Cited by
-
Percutaneous nephrostomy versus antegrade double-J stent placement in the treatment of malignant obstructive uropathy: a cost-effectiveness analysis from the perspective of the Brazilian public health care system.Radiol Bras. 2019 Sep-Oct;52(5):305-311. doi: 10.1590/0100-3984.2018.0127. Radiol Bras. 2019. PMID: 31656347 Free PMC article.
-
Twist and shout: magnetic resonance imaging findings in ovarian torsion.Radiol Bras. 2019 Nov-Dec;52(6):397-402. doi: 10.1590/0100-3984.2018.0079. Radiol Bras. 2019. PMID: 32047334 Free PMC article.
-
Tomographic findings in Meckel's diverticulitis.Radiol Bras. 2019 Jul-Aug;52(4):272-273. doi: 10.1590/0100-3984.2017.0215. Radiol Bras. 2019. PMID: 31435091 Free PMC article. No abstract available.
-
Ureterolithiasis and the quest for rational use of diagnostic imaging methods.Radiol Bras. 2018 Nov-Dec;51(6):VII-VIII. doi: 10.1590/0100-3984.2018.51.6e2. Radiol Bras. 2018. PMID: 30559568 Free PMC article. No abstract available.
-
Prevalence of Urolithiasis by Ultrasonography Among Patients with Gout: A Cross-Sectional Study from the UP-Philippine General Hospital.Res Rep Urol. 2020 Sep 25;12:423-431. doi: 10.2147/RRU.S268700. eCollection 2020. Res Rep Urol. 2020. PMID: 33062621 Free PMC article.
References
-
- Mos C, Holt G, Iuhasz S, et al. The sensitivity of transabdominal ultrasound in the diagnosis of ureterolithiasis. Med Ultrason. 2010;12:188–197. - PubMed
-
- Hess B. Pathophysiology, diagnosis and conservative therapy in calcium kidney calculi. Ther Umsch. 2003;60:79–87. - PubMed
-
- Park SJ, Yi BH, Lee HK, et al. Evaluation of patients with suspected ureteral calculi using sonography as an initial diagnostic tool: how can we improve diagnostic accuracy? J Ultrasound Med. 2008;27:1441–1450. - PubMed
-
- Kamaya A, Wong-You-Cheong J, Park HS, et al. Diagnostic ultrasound: abdomen and pelvis. Philadelphia, PA: Elsevier; 2015.
-
- Ray AA, Ghiculete D, Pace KT, et al. Limitations to ultrasound in the detection and measurement of urinary tract calculi. Urology. 2010;76:295–300. - PubMed
LinkOut - more resources
Full Text Sources