Osteoid osteoma: Contemporary management
- PMID: 30370032
- PMCID: PMC6187004
- DOI: 10.4081/or.2018.7496
Osteoid osteoma: Contemporary management
Abstract
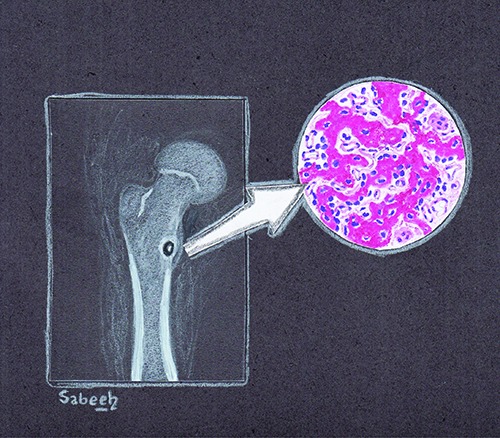
Osteoid osteoma is a benign bone-forming tumor with hallmark of tumor cells directly forming mature bone. Osteoid osteoma accounts for around 5% of all bone tumors and 11% of benign bone tumors with a male predilection. It occurs predominantly in long bones of the appendicular skeleton. According to Musculoskeletal Tumor Society staging system for benign tumors, osteoid osteoma is a stage-2 lesion. It is classified based on location as cortical, cancellous, or subperiosteal. Nocturnal pain is the most common symptom that usually responds to salicyclates and non-steroidal anti-inflammatory medications. CT is the modality of choice not only for diagnosis but also for specifying location of the lesion, i.e. cortical vs sub periosteal or medullary. Non-operative treatment can be considered as an option since the natural history of osteoid osteoma is that of spontaneous healing. Surgical treatment is an option for patients with severe pain and those not responding to NSAIDs. Available surgical procedures include radiofrequency (RF) ablation, CT-guided percutaneous excision and en bloc resection.
Keywords: Osteoid osteoma; benign; imaging; management; pathogenesis; tumor.
Conflict of interest statement
Conflict of interest: the authors declare no conflicts of interests.
Figures




References
-
- Greenspan A. Benign bone-forming lesions: osteoma, osteoid osteoma, and osteoblastoma. Skelet Radiol 1993;22:485-500. - PubMed
-
- Jaffe HL. Osteoid-osteoma: a benign osteoblastic tumor composed of osteoid and atypical bone. Archiv Surg 1935;31:709-28.
-
- Lee EH, Shafi M, Hui JH. Osteoid osteoma: a current review. J Pediatr Orthop 2006;26:695-700. - PubMed
-
- Kitsoulis P, Mantellos G, Vlychou M. Osteoid osteoma. Acta Orthop Belg 2006;72:119-25. - PubMed
-
- Ward WG, Eckardt JJ, Shayestehfar S, et al. Osteoid osteoma diagnosis and management with low morbidity. Clin Orthop Relat Res 1993;291:229-35. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials