

Editorial
doi: 10.21037/jtd.2018.07.136.
Scientific statement on spontaneous coronary artery dissection: care must be taken not to miss the association of spontaneous coronary artery dissection and takotsubo syndrome
Affiliations
- PMID: 30370106
- PMCID: PMC6186620
- DOI: 10.21037/jtd.2018.07.136
Item in Clipboard
Editorial
Scientific statement on spontaneous coronary artery dissection: care must be taken not to miss the association of spontaneous coronary artery dissection and takotsubo syndrome
J Thorac Dis.
2018 Sep.
No abstract available
Conflict of interest statement
Conflicts of Interest: The author has no conflicts of interest to declare.
Figures
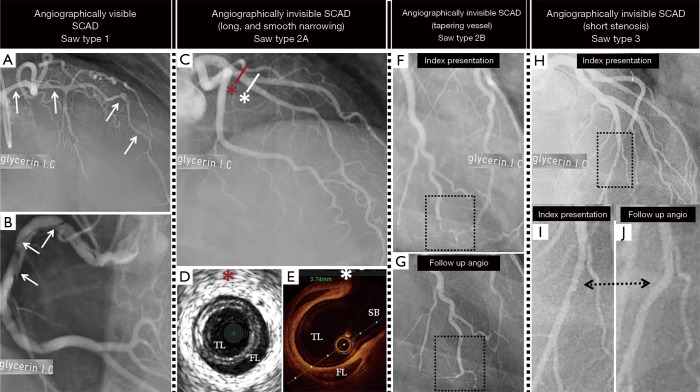
The figure demonstrates the coronary angiographic classification and the approach to diagnose SCAD. In angiographically visible SCAD, the CAG shows the pathognomonic signs of dissection as radiolucent intimal flap, dual or multiple lumens of different opacities, and contrast staining of the vessel wall (A, left coronary artery; B, right coronary artery, white arrows). The angiographically invisible SCAD may show a long smooth stenosis (type 2A) (C). If SCAD is in the proximal segments, the diagnosis may be confirmed by either IVUS showing the TL and the FL (D), or by OCT also showing the TL or FL (E). Note that the red asterisk in (C) indicates the level of LAD, which IVUS image in (D) is taken; White asterisk indicate the level of LAD in (C), which OCT image in (E) is taken. The angiographically invisible SCAD may involve the peripheral segments of the vessel and may be seen as “normal tapering vessel” (F, the SCAD lesion is shown in the dotted rectangle). The diagnosis is usually confirmed by follow up CAG after 6–8 weeks where there will be angiographic healing of the dissected vessel (G, the healed SCAD lesion is sown in the dotted rectangle). The invisible SCAD may also present as short stenosis resembling that of atherosclerotic coronary lesions (type 3) (H, The short SCAD lesion is shown in the dotted rectangle). The diagnosis of this type of SCAD may also be confirmed during follow up CAG as seen in the figure (I, during SCAD, and J during follow-up angiography). The diagnosis of the last type may also be confirmed by IVUS or OCT imaging. Type 1, 2A, 2B, and 3 are according to Saw classification (1). SCAD, spontaneous coronary artery dissection; CAG, coronary angiography; IVUS, intravascular ultrasound; TL, true lumen; FL, false lumen; OCT, optical coherence tomography.
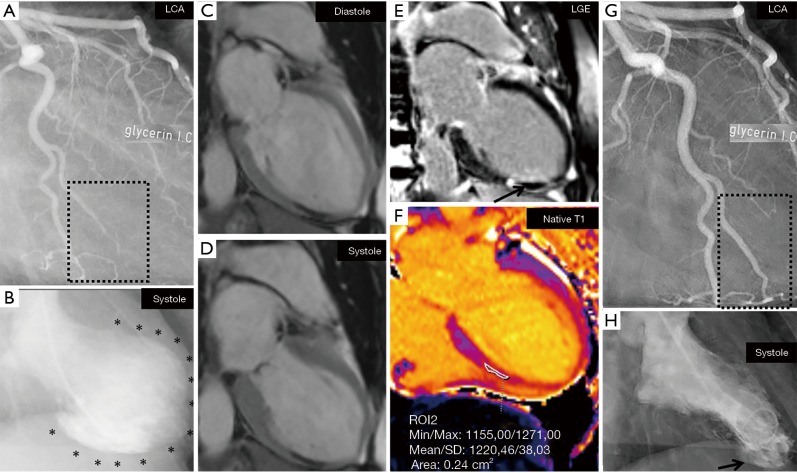
This figure illustrates the cardiac image study findings in a 54-year-old woman who presented with the clinical features of acute coronary syndrome. Acute invasive CAG revealed an obtuse-marginal (OM) branch stenosis and occlusion, which showed to be angiographically invisible SCAD (A, the OM SCAD lesion is shown in the dotted rectangle). Contrast left ventriculography shows LVWMA in the mid-apical region with good basal contractility resulting in a mid-apical ballooning and extending beyond the supply region of the OM artery (B, the black asterisks indicate the mid-apical ballooning of the left ventricle). The LVWMA and the mid-apical ballooning in a circumferential pattern was confirmed with CMR imaging (C, diastole; D, systole). There was sign of myocardial infarction with LGE corresponding to the OM supply region (E, black arrow) but no LGE in the remainder of the hypokinetic segments (E). In the hypokinetic segments with no LGE, there was increased Native T1 indicating edema (F). There was complete angiographic resolution of the dissected OM branch (G, the healed OM artery is shown in the dotted rectangle) during follow up CAG. Follow up left ventriculography revealed recovery of the LVWMA except in the infarcted region (H, black arrow). The findings are consistent with OM SCAD causing a limited myocardial infarction and inducing PIMS with features typical for TS. This patient has been published (18) but the figure is a new one. LVWMA, left ventricular wall motion abnormality; SCAD, spontaneous coronary artery dissection; CAG, coronary angiography; LGE, late gadolinium enhancement.
Comment on
-
Spontaneous Coronary Artery Dissection: Current State of the Science: A Scientific Statement From the American Heart Association.Circulation. 2018 May 8;137(19):e523-e557. doi: 10.1161/CIR.0000000000000564. Epub 2018 Feb 22. Circulation. 2018. PMID: 29472380 Free PMC article. Review.
References
Publication types
LinkOut - more resources
Full Text Sources