

Heart-lung interactions during mechanical ventilation: the basics
- PMID: 30370276
- PMCID: PMC6186561
- DOI: 10.21037/atm.2018.04.29
Heart-lung interactions during mechanical ventilation: the basics
Abstract
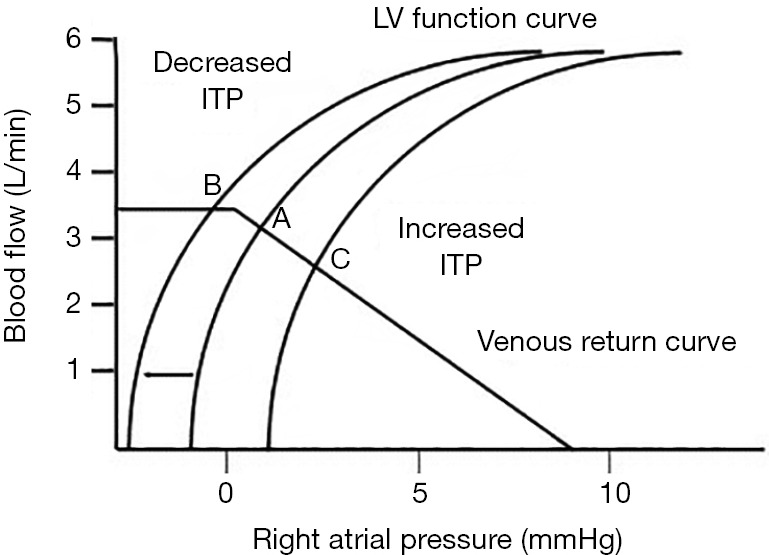
The hemodynamic effects of mechanical ventilation can be grouped into three clinically relevant concepts. First, since spontaneous ventilation is exercise. In patients increased work of breathing, initiation of mechanical ventilatory support may improve O2 delivery because the work of breathing is reduced. Second, changes in lung volume alter autonomic tone, pulmonary vascular resistance, and at high lung volumes compress the heart in the cardiac fossa similarly to cardiac tamponade. As lung volume increases so does the pressure difference between airway and pleural pressure. When this pressure difference exceeds pulmonary artery pressure, pulmonary vessels collapse as they pass form the pulmonary arteries into the alveolar space increasing pulmonary vascular resistance. Hyperinflation increases pulmonary vascular resistance impeding right ventricular ejection. Anything that over distends lung units will increase their vascular resistance, and if occurring globally throughout the lung, increase pulmonary vascular resistance. Decreases in end-expiratory lung volume cause alveolar collapse increases pulmonary vasomotor tone by the process of hypoxic pulmonary vasoconstriction. Recruitment maneuvers that restore alveolar oxygenation without over distention will reduce pulmonary artery pressure. Third, positive-pressure ventilation increases intrathoracic pressure. Since diaphragmatic descent increases intra-abdominal pressure, the decrease in the pressure gradient for venous return is less than would otherwise occur if the only change were an increase in right atrial pressure. However, in hypovolemic states, it can induce profound decreases in venous return. Increases in intrathoracic pressure decreases left ventricular afterload and will augment left ventricular ejection. In patients with hypervolemic heart failure, this afterload reducing effect can result in improved left ventricular ejection, increased cardiac output and reduced myocardial O2 demand. This brief review will focus primarily on mechanical ventilation and intrathoracic pressure as they affect right and left ventricular function and cardiac output.
Keywords: Afterload; heart-lung interactions; preload; ventricular interdependence.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
-
- Sette P, Dorizzi RM, Azzini AM. Vascular access: an historical perspective from Sir William Harvey to the 1956 Nobel prize to Andre F. Cournand, Werner Forssmann, and Dickinson W. Richards. J Vasc Access 2012;13:137-44. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials