

Dose escalation for locally advanced pancreatic cancer: How high can we go?
- PMID: 30370371
- PMCID: PMC6200902
- DOI: 10.1016/j.adro.2018.07.008
Dose escalation for locally advanced pancreatic cancer: How high can we go?
Abstract
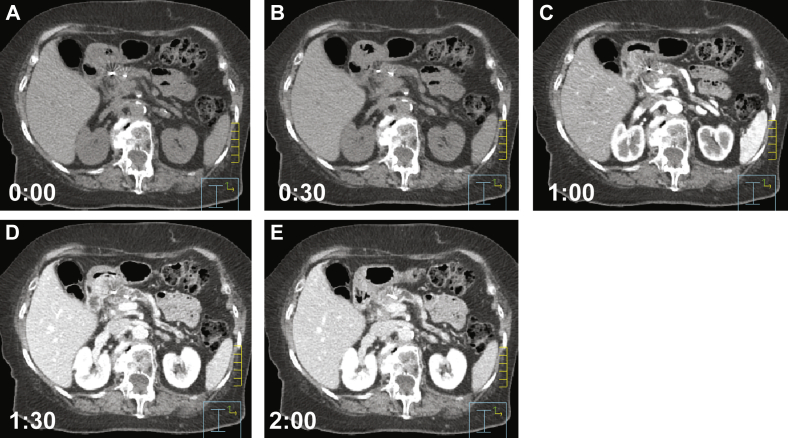
Purpose: There are limited treatment options for locally advanced, unresectable pancreatic cancer (LAPC) and no likelihood of cure without surgery. Radiation offers an option for local control, but radiation dose has previously been limited by nearby bowel toxicity. Advances in on-board imaging and treatment planning may allow for dose escalation not previously feasible and improve local control. In preparation for development of clinical trials of dose escalation in LAPC, we undertook a dosimetric study to determine the maximum possible dose escalation while maintaining known normal tissue constraints.
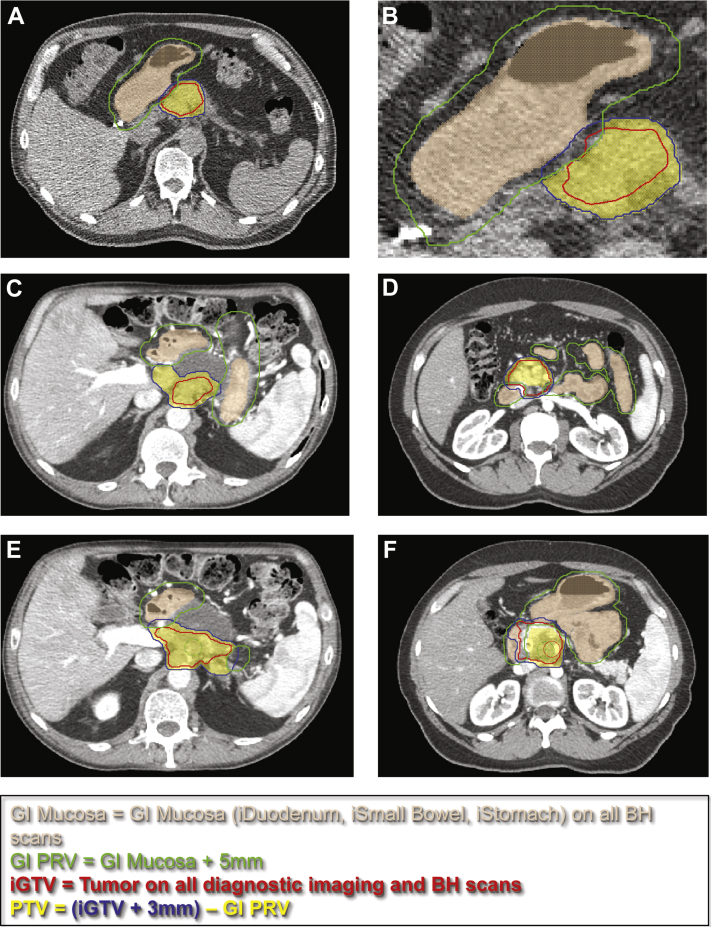
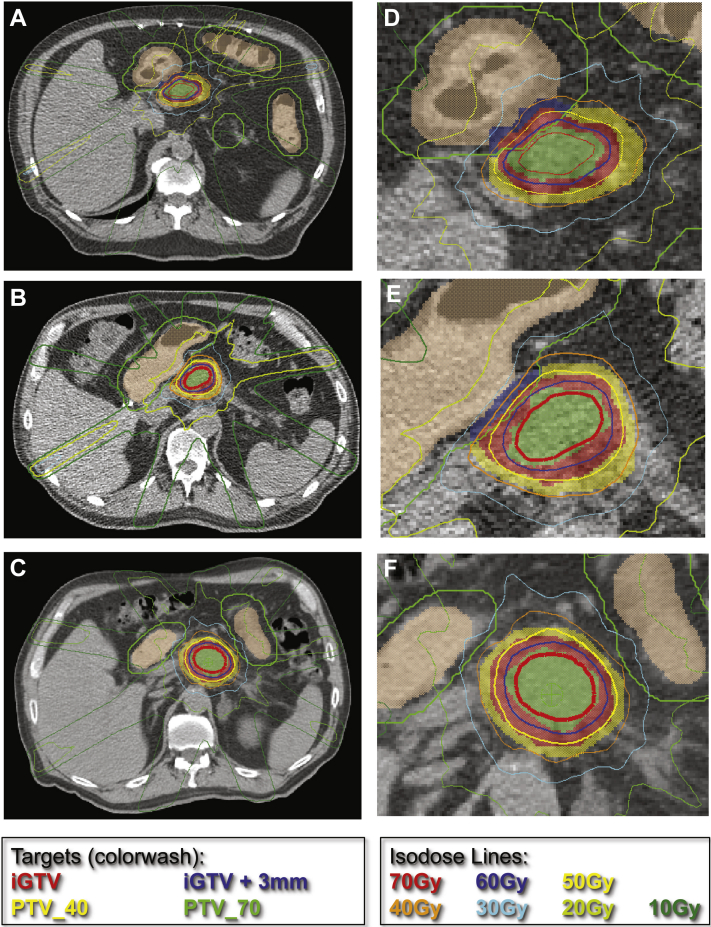
Methods and materials: Twenty patients treated at our institution with either SBRT or dose-escalated hypofractionated IMRT (DE-IMRT) were re-planned using dose escalated SBRT to 70 Gy in 5 fractions to the GTV and 40 Gy in 5 fractions to the PTV. Standard accepted organ at risk (OAR) constraints were used for planning. Descriptive statistics were generated for homogeneity, conformality, OAR's and GTV/PTV.
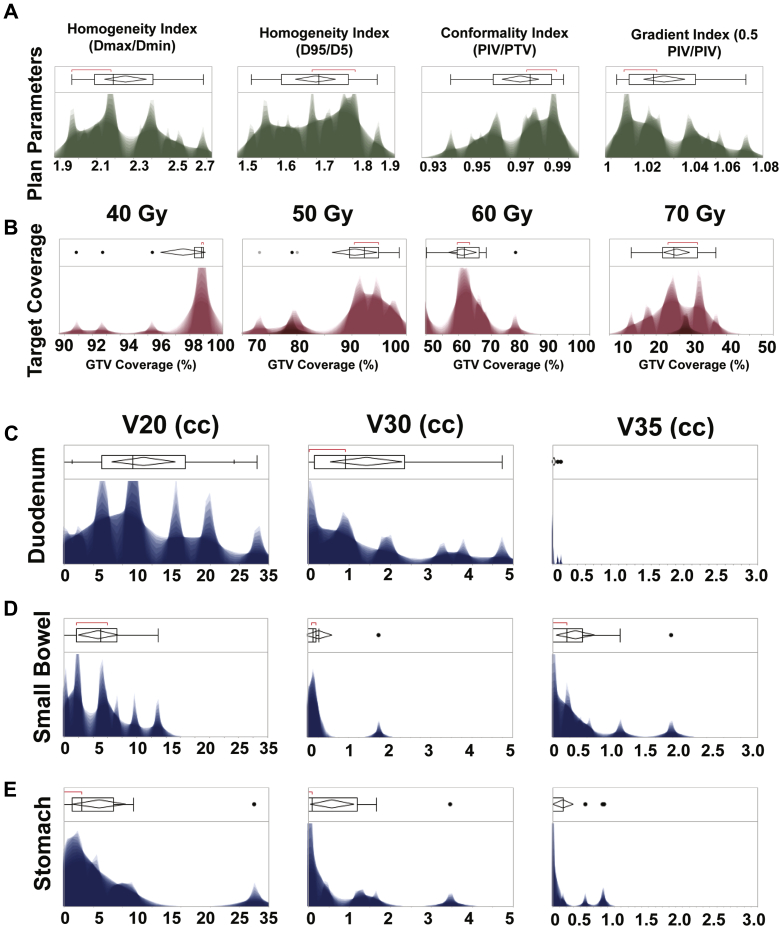
Results: Mean iGTV coverage by 50 Gy was 91% (±0.07%), by 60 Gy was 61.3% (±0.08%) and by 70 Gy was 24.4% (±0.05%). Maximum PTV coverage by 70 Gy was 33%. Maximum PTV coverage by 60 Gy was 77.5%. The following organ at risk (OAR) constraints were achieved for 90% of generated plans: Duodenum V20 < 30 cc, V30 < 3 cc, V35 < 1 cc; Small Bowel V20 < 15 cc, V30 < 1 cc, V35 < 0.1 cc; Stomach V20 < 20 cc, V30 < 2 cc, V35 < 1 cc. V40 < 0.5 cc was achieved for all OAR.
Conclusions: Dose escalation to 60 Gy is dosimetrically feasible with adequate GTV coverage. The identified constraints for OAR's will be used in ongoing clinical trials.
Figures
References
-
- Conroy T., Desseigne F., Ychou M. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med. 2011;364:1817–1825. - PubMed
-
- Hammel P., Huguet F., van Laethem J.L. Effect of chemoradiotherapy vs chemotherapy on survival in patients with locally advanced pancreatic cancer controlled after 4 months of gemcitabine with or without erlotinib: The LAP07 randomized clinical trial. JAMA. 2016;315:1844–1853. - PubMed
LinkOut - more resources
Full Text Sources
