

Missed Opportunities for Screening and Surveillance of Barrett's Esophagus in Veterans with Esophageal Adenocarcinoma
- PMID: 30370493
- PMCID: PMC6358496
- DOI: 10.1007/s10620-018-5336-5
Missed Opportunities for Screening and Surveillance of Barrett's Esophagus in Veterans with Esophageal Adenocarcinoma
Abstract
Background: Barrett's esophagus (BE) is the premalignant lesion of esophageal adenocarcinoma (EAC) and is the target of early detection and prevention efforts for EAC.
Aims: We sought to evaluate what proportion and temporal trends of EAC patients had missed opportunities for screening and surveillance of BE.
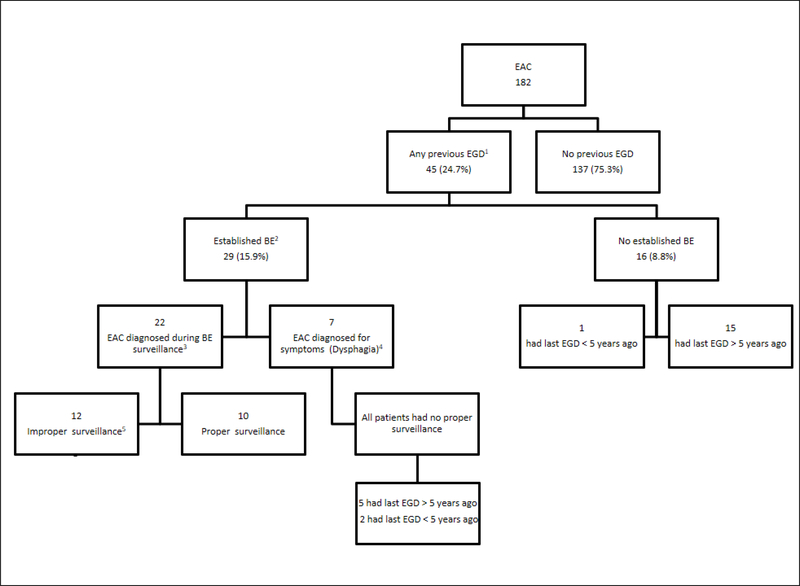
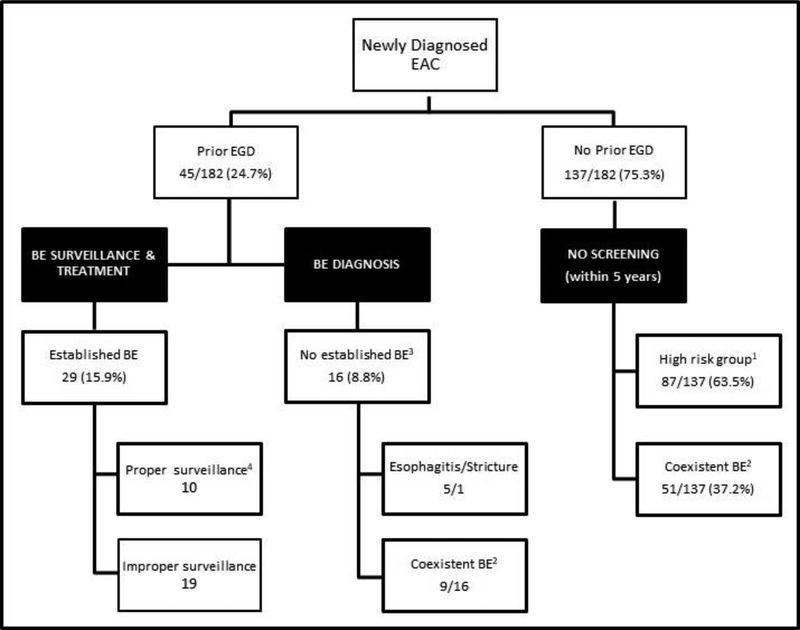
Methods: Our study included 182 patients with EAC at the Michael E. DeBakey VA Medical Center in Houston, Texas, between 02/2005 and 09/2017. We conducted a retrospective audit of patients' medical records for any previous upper endoscopies (EGDs) for screening or surveillance of BE prior to their EAC diagnosis.
Results: The mean age of the cohort was 67.3 years (SD = 9.5); 99.5% of patients were male, and 85.2% were white. Only 45 patients (24.7%) had EGD at any time prior to the cancer diagnosing EGD, of whom 29 (15.9% of all EAC cases) had an established BE diagnosis. In the 137 patients with no prior EGD, most (63.5%) had GERD or were obese or ever smokers. There were no changes in patterns over time. For the 29 patients with prior established BE, 22 (75.8%) were diagnosed with EAC as a result of surveillance EGD. Patients with prior established BE were more likely to be diagnosed at 0 or I stage (p < 0.001) and managed with endoscopic or surgical modalities (p < 0.001) than patients without prior BE.
Conclusions: Despite having established risk factors for BE, the majority of EAC patients had no prior EGD to screen for BE. BE screening may represent the largest missed opportunity to reduce EAC mortality.
Keywords: Barrett’s esophagus; Esophageal adenocarcinoma; Esophagogastroduodenoscopy (EGD); GERD; Guidelines; Quality improvement; Screening and surveillance.
Conflict of interest statement
Figures
References
-
- Thrift AP and Whiteman DC, The incidence of esophageal adenocarcinoma continues to rise: analysis of period and birth cohort effects on recent trends. Annals of Oncology, 2012. 23(12): p. 3155–3162. - PubMed
-
- Rustgi AK and El-Serag HB, Esophageal Carcinoma. New England Journal of Medicine, 2014. 371(26): p. 2499–2509. - PubMed
-
- Thrift AP, The epidemic of oesophageal carcinoma: Where are we now? Cancer Epidemiology, 2016. 41: p. 88–95. - PubMed
-
- Maret-Ouda J, El-Serag HB, and Lagergren J, Opportunities for Preventing Esophageal Adenocarcinoma. Cancer Prevention Research, 2016. 9(11): p. 828–834. - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
