

Challenges in Prenatal Treatment with Dexamethasone
- PMID: 30371037
- PMCID: PMC6786883
- DOI: 10.17458/per.vol16.2018.mcpa.dexamethasone
Challenges in Prenatal Treatment with Dexamethasone
Abstract
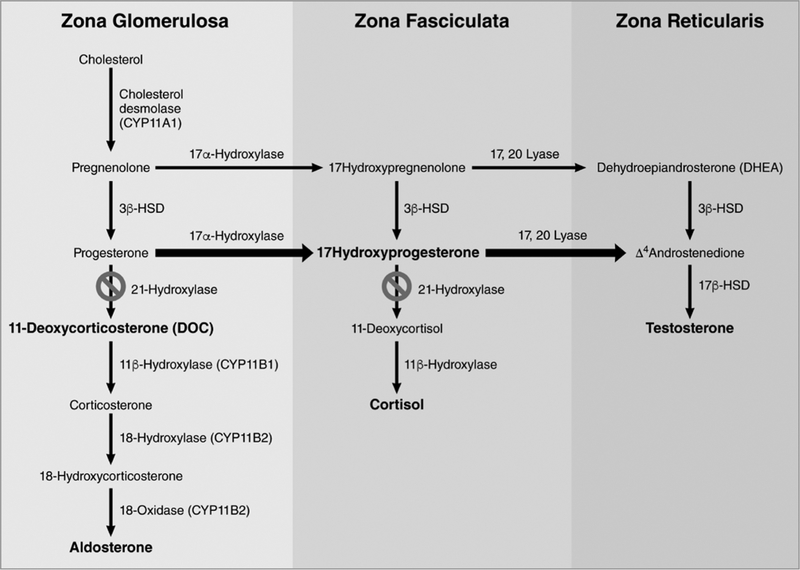
Classic congenital adrenal hyperplasia (CAH) due to 21-hydroxylase deficiency causes elevated androgen levels, which can lead to virilization of female external genitalia. Prenatal dexamethasone treatment has been shown to be effective in preventing virilization of external genitalia when started prior to 7-9 weeks of gestation in females with classic CAH. However, CAH cannot be diagnosed prenatally until the end of the first trimester. Treating pregnant women with a fetus at risk of developing classic CAH exposes a significant proportion of fetuses unnecessarily, because only 1 in 8 would benefit from treatment. Consequently, prenatal dexamethasone treatment has been met with much controversy due to the potential adverse outcomes when exposed to high-dose steroids in utero. Here, we review the short- and long-term outcomes for fetuses and pregnant women exposed to dexamethasone treatment, the ethical considerations that must be taken into account, and current practice recommendations.
Keywords: Congenital Adrenal Hyperplasia; Ethics; Prenatal; Treatment.
Copyright© of YS Medical Media ltd.
Figures


Similar articles
-
Congenital adrenal hyperplasia: update on prenatal diagnosis and treatment.J Steroid Biochem Mol Biol. 1999 Apr-Jun;69(1-6):19-29. doi: 10.1016/s0960-0760(99)00059-x. J Steroid Biochem Mol Biol. 1999. PMID: 10418977 Review.
-
Prenatal diagnosis and treatment of 11beta-hydroxylase deficiency congenital adrenal hyperplasia resulting in normal female genitalia.J Clin Endocrinol Metab. 1999 Sep;84(9):3129-34. doi: 10.1210/jcem.84.9.5976. J Clin Endocrinol Metab. 1999. PMID: 10487675
-
Prenatal diagnosis for congenital adrenal hyperplasia in 532 pregnancies.J Clin Endocrinol Metab. 2001 Dec;86(12):5651-7. doi: 10.1210/jcem.86.12.8072. J Clin Endocrinol Metab. 2001. PMID: 11739415
-
Prenatal dexamethasone treatment in pregnancies at risk for congenital adrenal hyperplasia due to 21-hydroxylase deficiency: effect on midgestational amniotic fluid steroid levels.J Clin Endocrinol Metab. 1993 Jan;76(1):117-20. doi: 10.1210/jcem.76.1.8421074. J Clin Endocrinol Metab. 1993. PMID: 8421074
-
Prenatal Treatment with Dexamethasone in Suspected Congenital Adrenal Hyperplasia and Orofacial Cleft: a Case Report and Review of the Literature.Pediatr Endocrinol Rev. 2017 Sep;15(1):21-25. doi: 10.17458/per.vol15.2017.rvc.prenataltreatment. Pediatr Endocrinol Rev. 2017. PMID: 28845624 Review.
Cited by
-
Dexamethasone exposure during pregnancy triggers metabolic syndrome in offspring via epigenetic alteration of IGF1.Cell Commun Signal. 2024 Jan 23;22(1):62. doi: 10.1186/s12964-024-01472-6. Cell Commun Signal. 2024. PMID: 38263047 Free PMC article.
-
First Trimester Dexamethasone Treatment Is Not Associated With Alteration in Resting-state Connectivity at Adolescent or Adult Age.J Clin Endocrinol Metab. 2022 Sep 28;107(10):2769-2776. doi: 10.1210/clinem/dgac426. J Clin Endocrinol Metab. 2022. PMID: 35882216 Free PMC article.
-
Integrated Profiling Identifies Long-Term Molecular Consequences of Prenatal Dexamethasone Treatment in the Rat Brain-Potential Triggers of Depressive Phenotype and Cognitive Impairment.Mol Neurobiol. 2025 Apr;62(4):5183-5201. doi: 10.1007/s12035-024-04586-7. Epub 2024 Nov 11. Mol Neurobiol. 2025. PMID: 39528842 Free PMC article.
-
Evaluation of cross-platform compatibility of a DNA methylation-based glucocorticoid response biomarker.Clin Epigenetics. 2022 Oct 28;14(1):136. doi: 10.1186/s13148-022-01352-1. Clin Epigenetics. 2022. PMID: 36307860 Free PMC article.
-
Advancing precision care in pregnancy through a treatable fetal findings list.Am J Hum Genet. 2025 Jun 5;112(6):1251-1269. doi: 10.1016/j.ajhg.2025.03.011. Epub 2025 Apr 9. Am J Hum Genet. 2025. PMID: 40209713 Review.
References
-
- Speiser PW, Azziz R, Baskin LS, Ghizzoni L, Hensle TW, Merke DP, Meyer-Bahlburg HF, Miller WL, Montori VM, Oberfield SE, Ritzen M, White PC, Endocrine S. Congenital adrenal hyperplasia due to steroid 21-hydroxylase deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 2010;95(9):4133–4160 - PMC - PubMed
-
- David M, Forest MG. Prenatal treatment of congenital adrenal hyperplasia resulting from 21-hydroxylase deficiency. J Pediatr 1984;105(5):799–803 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous