

Predicting Bleeding Events in Anticoagulated Patients With Atrial Fibrillation: A Comparison Between the HAS-BLED and GARFIELD-AF Bleeding Scores
- PMID: 30371183
- PMCID: PMC6222935
- DOI: 10.1161/JAHA.118.009766
Predicting Bleeding Events in Anticoagulated Patients With Atrial Fibrillation: A Comparison Between the HAS-BLED and GARFIELD-AF Bleeding Scores
Abstract
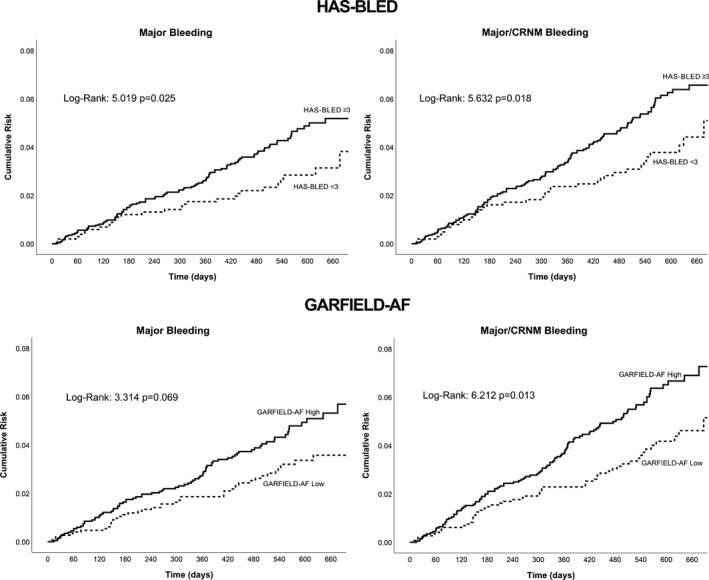
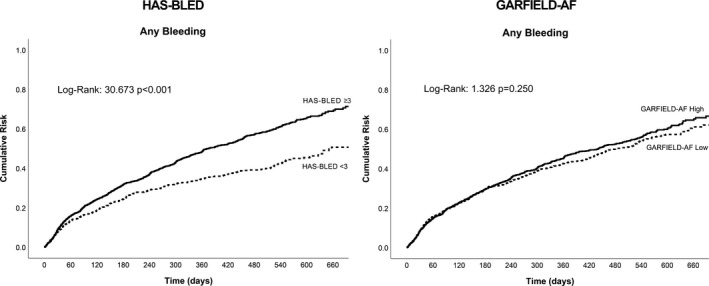
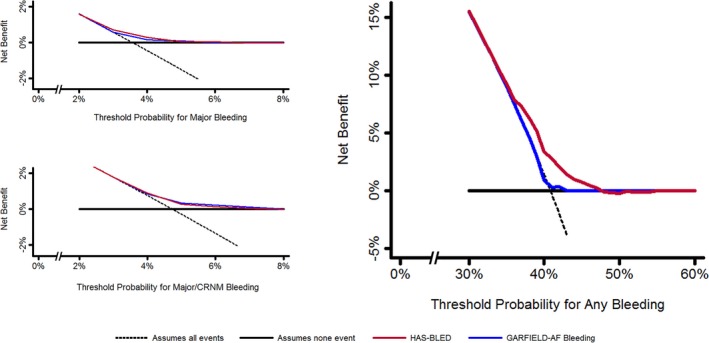
Background Patients with atrial fibrillation (AF) treated with oral anticoagulants may be exposed to an increased risk of bleeding events. The HAS-BLED (Hypertension, Abnormal renal and liver function, Stroke, Bleeding, Labile INRs, Elderly, Drugs or alcohol) score is a simple, well-established, clinical bleeding-risk prediction score. Recently, a new algorithm-based score was proposed, the GARFIELD-AF (Global Anticoagulant in the Field-AF) bleeding score. We compared HAS-BLED and GARFIELD-AF scores in predicting adjudicated bleeding events in a clinical trial cohort of patients with AF taking anticoagulants, in the first external comparative validation of both scores. Methods and Results We analyzed patients from the SPORTIF (Stroke Prevention Using an Oral Thrombin Inhibitor in Patients With AF) III and V trials. All patients assigned to the warfarin arm with information to calculate the scores were considered. Outcomes were major, major/clinically relevant nonmajor, and any bleeding. A total of 3550 warfarin-treated patients were available for analysis. Of these patients, 2519 (71.0%) had a HAS-BLED score ≥3, whereas based on GARFIELD-AF median value, 2056 (57.9%) were categorized as "high score." Both HAS-BLED and GARFIELD-AF C-indexes showed modest predictive value (C-index [95% confidence interval] for major bleeding, 0.58 [0.56-0.60] and 0.56 [0.54-0.57], respectively); however, GARFIELD-AF was not predictive of any bleeding. The GARFIELD-AF bleeding score had a significantly lower sensitivity and a negative reclassification for any bleeding compared with HAS-BLED, assessed by integrated discrimination improvement and net reclassification improvement (both P<0.001). HAS-BLED showed a 5% net benefit for any bleeding occurrence. Conclusions The algorithm-based GARFIELD-AF bleeding score did not show any significant improvement in major and major/clinically relevant nonmajor prediction compared with the simple HAS-BLED score. For clinical usefulness in prediction of any bleeding, the HAS-BLED score showed a significant net benefit compared with the GARFIELD-AF.
Keywords: atrial fibrillation; bleeding risk; clinical risk scores.
Figures
Comment in
-
Bleeding Risk Scores in Atrial Fibrillation: Helpful or Harmful?J Am Heart Assoc. 2018 Sep 18;7(18):e010582. doi: 10.1161/JAHA.118.010582. J Am Heart Assoc. 2018. PMID: 30371216 Free PMC article. No abstract available.
References
-
- Lip GYH, Freedman B, de Caterina R, Potpara TS. Stroke prevention in atrial fibrillation: past, present and future comparing the guidelines and practical decision‐making. Thromb Haemost. 2017;117:1230–1239. - PubMed
-
- Lamberts M, Staerk L, Olesen JB, Fosbøl EL, Hansen ML, Harboe L, Lefevre C, Evans D, Gislason GH. Major bleeding complications and persistence with oral anticoagulation in non‐valvular atrial fibrillation: contemporary findings in real‐life Danish patients. J Am Heart Assoc. 2017;6:e004517 DOI: 10.1161/JAHA.116.004517. - DOI - PMC - PubMed
-
- Lip GYH, Andreotti F, Fauchier L, Huber K, Hylek E, Knight E, Lane D, Levi M, Marin F, Palareti G, Kirchhof P. Bleeding risk assessment and management in atrial fibrillation patients: executive summary of a position document from the European Heart Rhythm Association [EHRA], endorsed by the European Society of Cardiology [ESC] working group on thrombosis. Thromb Haemost. 2011;106:997–1011. - PubMed
-
- Kirchhof P, Benussi S, Kotecha D, Ahlsson A, Atar D, Casadei B, Castella M, Diener H‐C, Heidbuchel H, Hendriks J, Hindricks G, Manolis AS, Oldgren J, Popescu BA, Schotten U, Van Putte B, Vardas P, Agewall S, Camm J, Baron Esquivias G, Budts W, Carerj S, Casselman F, Coca A, De Caterina R, Deftereos S, Dobrev D, Ferro JM, Filippatos G, Fitzsimons D, Gorenek B, Guenoun M, Hohnloser SH, Kolh P, Lip GYH, Manolis A, McMurray J, Ponikowski P, Rosenhek R, Ruschitzka F, Savelieva I, Sharma S, Suwalski P, Tamargo JL, Taylor CJ, Van Gelder IC, Voors AA, Windecker S, Zamorano JL, Zeppenfeld K. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur Heart J. 2016;37:2893–2962. - PubMed
-
- Chao T‐F, Lip GYH, Lin Y‐J, Chang S‐L, Lo L‐W, Hu Y‐F, Tuan T‐C, Liao J‐N, Chung F‐P, Chen T‐J, Chen S‐A. Incident risk factors and major bleeding in patients with atrial fibrillation treated with oral anticoagulants: a comparison of baseline, follow‐up and Delta HAS‐BLED scores with an approach focused on modifiable bleeding risk factors. Thromb Haemost. 2018;118:768–777. - PubMed
