

Life Course Trajectories of Cardiovascular Risk Factors in Women With and Without Hypertensive Disorders in First Pregnancy: The HUNT Study in Norway
- PMID: 30371249
- PMCID: PMC6201453
- DOI: 10.1161/JAHA.118.009250
Life Course Trajectories of Cardiovascular Risk Factors in Women With and Without Hypertensive Disorders in First Pregnancy: The HUNT Study in Norway
Abstract
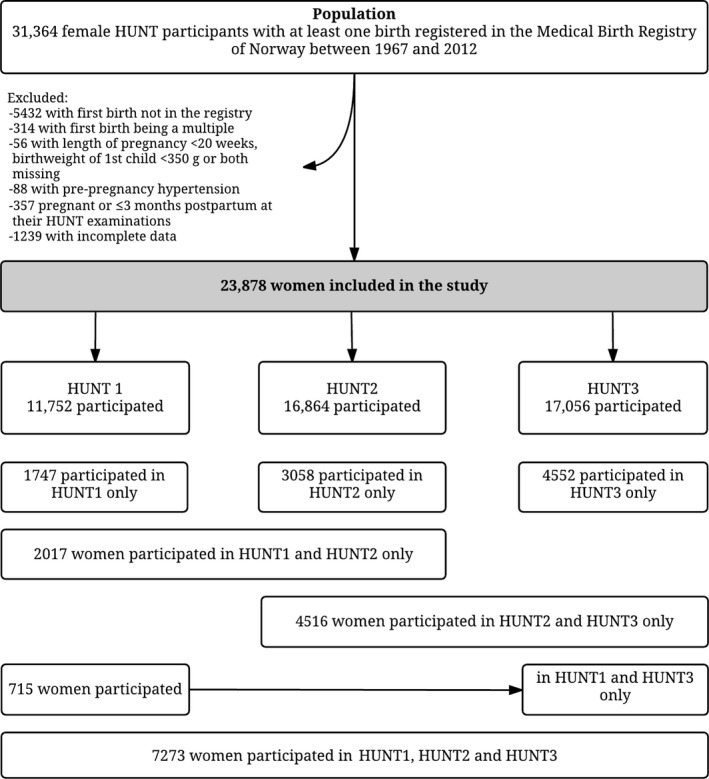
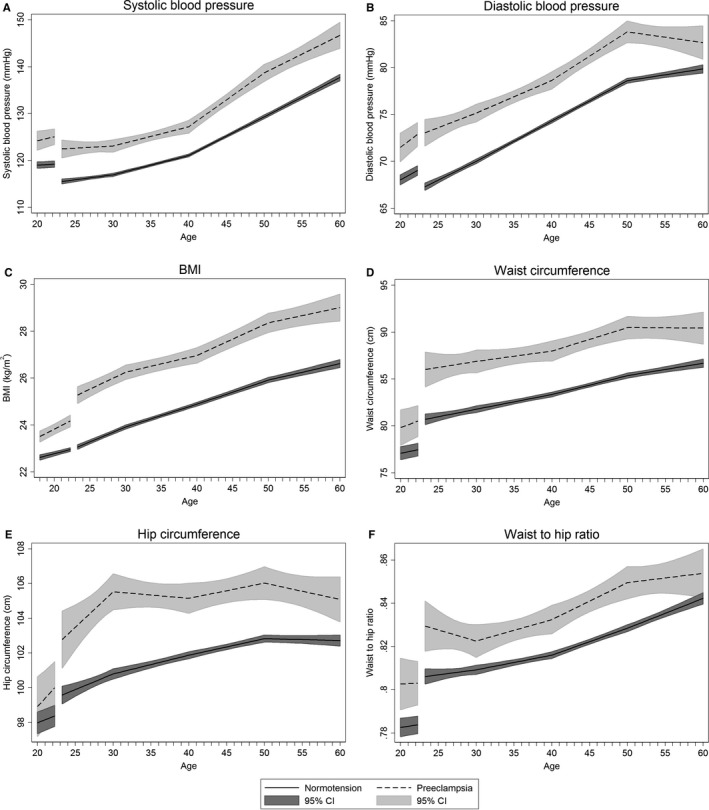
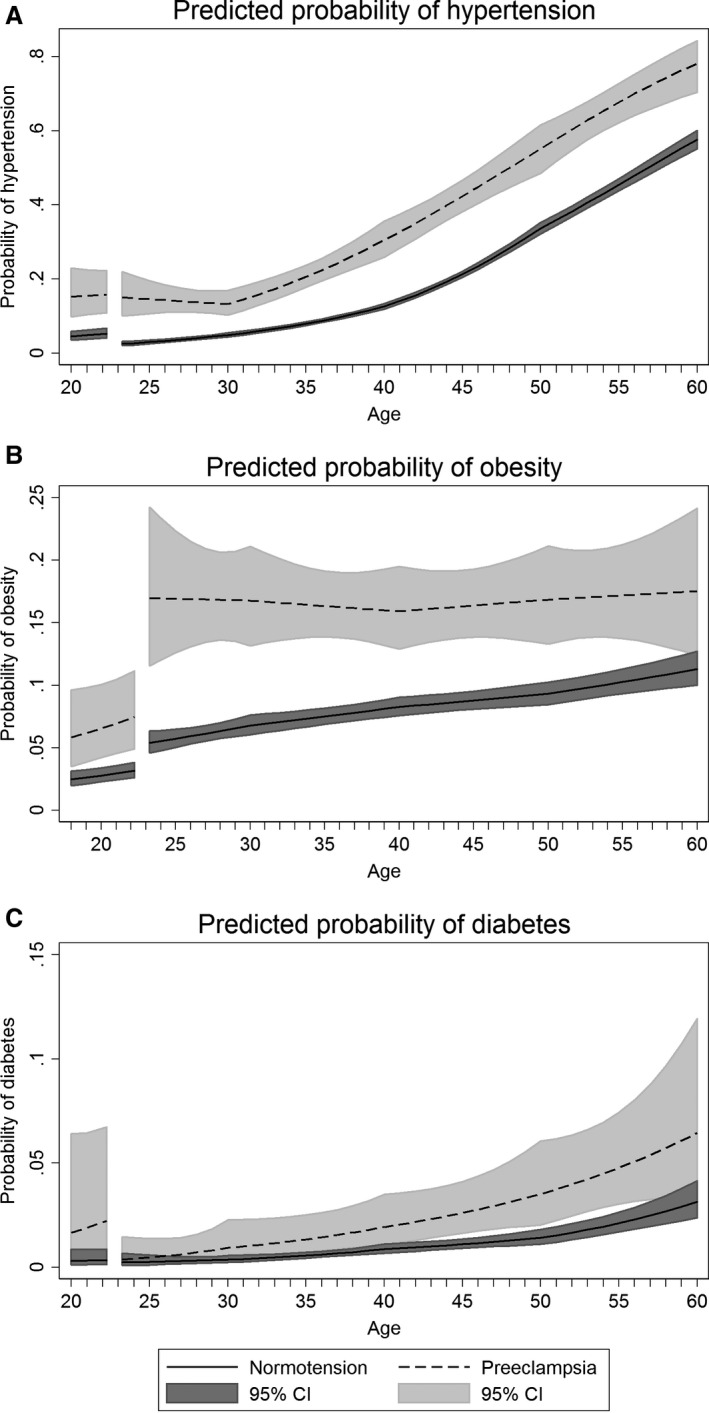
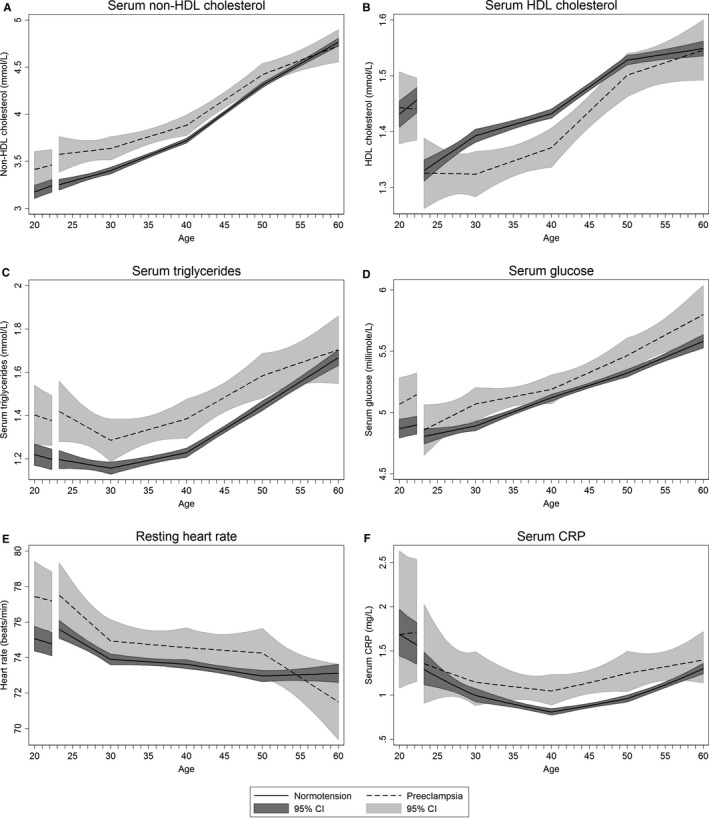
Background Women with hypertensive pregnancy disorders have adverse levels of cardiovascular risk factors. It is unclear how this adverse risk factor profile evolves during adult life. We compared life course trajectories of cardiovascular risk factors in women with preeclampsia or gestational hypertension in their first pregnancy to normotensive women. Methods and Results We linked information on cardiovascular risk factors from the population-based HUNT (Nord-Trøndelag Health Study) surveys with pregnancy information from the Medical Birth Registry of Norway. Trajectories of cardiovascular risk factors were constructed for 22 308 women with a normotensive first pregnancy; 1092 with preeclampsia, and 478 with gestational hypertension in first pregnancy. Already before first pregnancy, women with preeclampsia in their first pregnancy had higher measures of adiposity, blood pressure, heart rate, and serum lipids and glucose compared with women with a normotensive first pregnancy. After first pregnancy, there was a parallel development in cardiovascular risk factor levels, but women with a normotensive first pregnancy had a time lag of >10 years compared with the preeclampsia group. There were no clear differences in risk factor trajectories between women with gestational hypertension and women with preeclampsia. Conclusions Women with hypertensive pregnancy disorders in their first pregnancy had an adverse cardiovascular risk factor profile before pregnancy compared with normotensive women, and the differences persisted beyond 50 years of age. Hypertensive disorders in pregnancy signal long-term increases in modifiable cardiovascular risk factors, and may be used to identify women who would benefit from early prevention strategies.
Keywords: cardiovascular risk factors; epidemiology; hypertensive disorders of pregnancy; life course.
Figures
References
-
- Gholizadeh L, Davidson P. More similarities than differences: an international comparison of CVD mortality and risk factors in women. Health Care Women Int. 2008;29:3–22. - PubMed
-
- American College of Obstetricians and Gynecologists . Hypertension in pregnancy. Report of the American College of Obstetricians and Gynecologists’ Task Force on Hypertension in Pregnancy. Obstet Gynecol. 2013;122:1122–1131. - PubMed
-
- Mosca L, Benjamin EJ, Berra K, Bezanson JL, Dolor RJ, Lloyd‐Jones DM, Newby LK, Piña IL, Roger VL, Shaw LJ, Zhao D, Beckie TM, Bushnell C, D'Armiento J, Kris‐Etherton PM, Fang J, Ganiats TG, Gomes AS, Gracia CR, Haan CK, Jackson EA, Judelson DR, Kelepouris E, Lavie CJ, Moore A, Nussmeier NA, Ofili E, Oparil S, Ouyang P, Pinn VW, Sherif K, Smith SC, Sopko G, Chandra‐Strobos N, Urbina EM, Vaccarino V, Wenger NK. Effectiveness‐based guidelines for the prevention of cardiovascular disease in women—2011 update. Circulation. 2011;123:1243–1262. - PMC - PubMed
-
- Piepoli MF, Hoes AW, Agewall S, Albus C, Brotons C, Catapano AL, Cooney M‐T, Corrà U, Cosyns B, Deaton C, Graham I, Hall MS, Hobbs FDR, Løchen M‐L, Löllgen H, Marques‐Vidal P, Perk J, Prescott E, Redon J, Richter DJ, Sattar N, Smulders Y, Tiberi M, van der Worp HB, van Dis I, Verschuren WMM; Authors/Task Force Members . 2016 European guidelines on cardiovascular disease prevention in clinical practice: the Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts). Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur Heart J. 2016;37:2315–2381. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
