

Review
doi: 10.1161/JAHA.118.009778.
Eradicating the Burden of Atherosclerotic Cardiovascular Disease by Lowering Apolipoprotein B Lipoproteins Earlier in Life
Affiliations
- PMID: 30371276
- PMCID: PMC6474943
- DOI: 10.1161/JAHA.118.009778
Item in Clipboard
Review
Eradicating the Burden of Atherosclerotic Cardiovascular Disease by Lowering Apolipoprotein B Lipoproteins Earlier in Life
J Am Heart Assoc.
.
No abstract available
Keywords: apolipoprotein; primary prevention; randomized trial; regression.
Figures
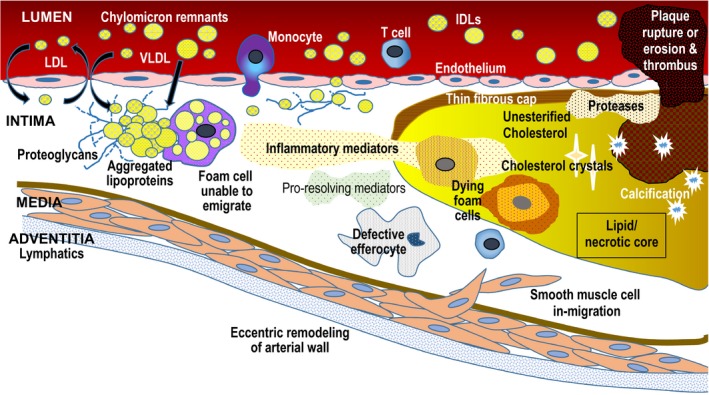
Apo B lipoprotein response‐to‐retention model of atherosclerosis initiation and progression. High plasma concentrations of apo B lipoproteins (LDL , IDL , VLDL , chylomicron remnants, Lp(a)) increase entry into intima and retention. Apo B lipoproteins bind to proteoglycans and begin aggregating, a process that accelerates once plaque begins. Retention is influenced by particle composition and diet, among other factors. Retention leads to a maladaptive cellular response leading to increased inflammation, fibrosis, and necrosis. The lipid/necrotic core forms when normal phagocytotic processes and efferocytosis are overwhelmed by continued retention and accumulation of “toxic” apo B lipoproteins. Plaque rupture or erosion can lead to formation of overlying thrombus, which can precipitate an acute clinical event. Apo indicates Apolipoprotein; IDL , intermediate lipoprotein; LDL , low‐density lipoprotein; Lp(a), Lipoprotein (a); VLDL , very‐low‐density lipoprotein.
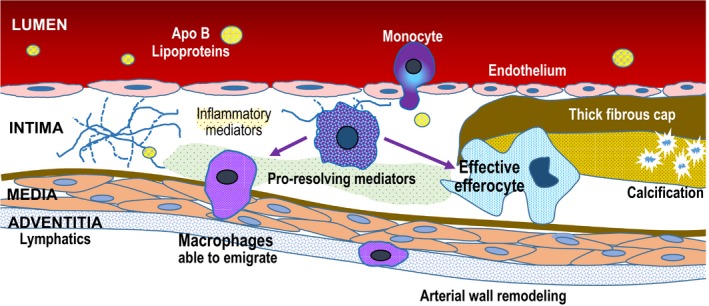
Mechanisms of regression following apo B lipoprotein reduction. Dramatic reduction in plasma concentrations of LDL ‐C and other apo B lipoproteins leads to decreased subendothelial entry and retention. Decreased levels of “toxic” apo B lipoproteins allows normal phagocytic and inflammation resolving mechanisms to “heal” the plaque. Decreased foam cell formation in the intima allows macrophages to migrate into adventitial lymphatics. Increased in‐migration of monocytes that become healthy macrophages results in effective efferocytosis to remove necrotic debris. Apo indicates apolipoprotein.
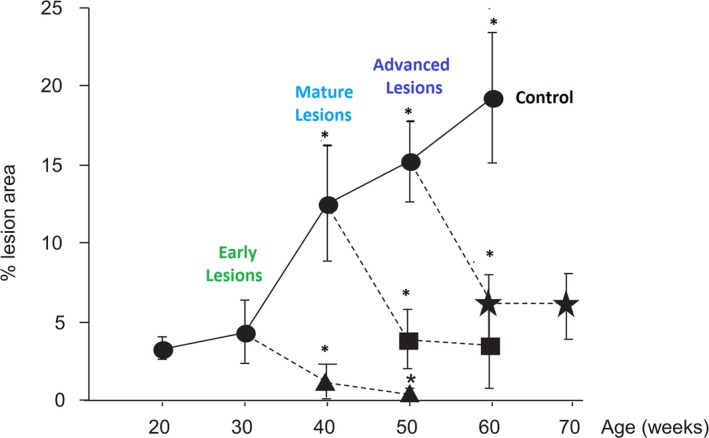
Complete regression of early plaque lesions when intensive cholesterol lowering to 11 to 55 mg/dL starts at 30 weeks, compared with substantial although not complete regression of later stages of plaque when intensive cholesterol lowering is initiated at 40 or 50 weeks. Adapted from Björkegren et al44 with permission. Copyright ©2014 PLOS Genetics. ***P<0.001.
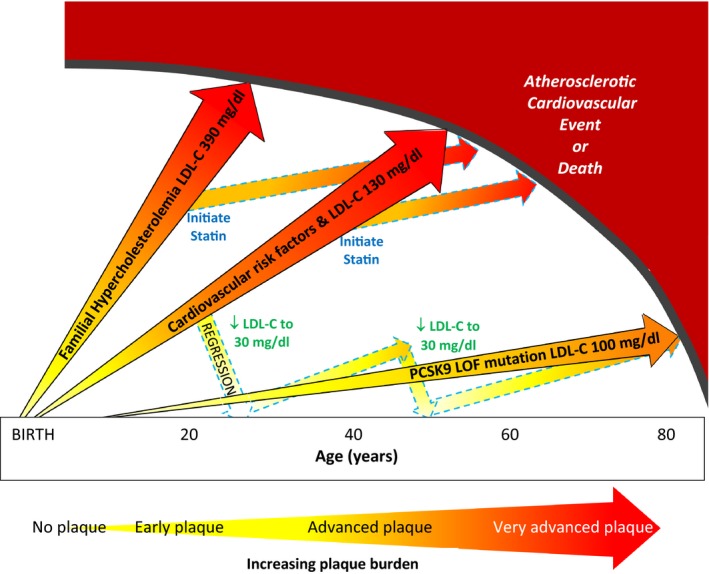
Life course trajectory of atherosclerotic progression is illustrated for individuals at very high, high, and low risk of atherosclerotic cardiovascular disease events (ASCVD ). (1) individuals with heterozygous familial hypercholesterolemia who have severe LDL ‐C elevation from birth have markedly accelerated atherosclerosis and premature onset of clinical ASCVD events; (2) individuals with cardiovascular risk factors from young adulthood and “average” LDL ‐C levels of 130 mg/dL are more likely to experience clinical ASCVD events in early and middle age; and (3) individuals with a proprotein convertase subtilisin/kexin type 9 PCSK 9 loss‐of‐function (PCSK 9 LOF ) mutation have lower LDL ‐C levels throughout the lifespan and may be at markedly reduced risk of clinical ASCVD events. LDL ‐C lowering with statins can stabilize and modestly regress plaque but does not eradicate the plaque burden and remain at increased risk of clinical ASCVD events. Intensive LDL ‐C lowering to 20 to 40 mg/dL may have a greater impact on plaque regression in earlier stages of plaque. A new paradigm of “regression” treatment with intensive LDL ‐C lowering earlier in the course of atherosclerosis or at younger ages could then be followed by intermittent retreatment to “maintain” a low plaque burden until late in life. LDL ‐C indicates low‐density lipoprotein cholesterol (to convert to mmol/L divide by 38.65 mg/dL); PCSK 9 LOF indicates proprotein convertase subtilisin/kexin type 9 loss‐of‐function mutation.
References
-
- Sidney S, Quesenberry CP Jr, Jaffe MG, Sorel M, Nguyen‐Huynh MN, Kushi LH, Go AS, Rana JS. Recent trends in cardiovascular mortality in the United States and public health goals. JAMA Cardiol. 2016;1:594–599. - PubMed
-
- Sniderman AD, Thanassoulis G, Williams K, Pencina M. Risk of premature cardiovascular disease vs the number of premature cardiovascular events. JAMA Cardiol. 2016;1:492–494. - PubMed
-
- Robinson JG, Huijgen R, Ray K, Persons J, Kastelein JJP, Pencina MJ. Determining when to add nonstatin therapy: a quantitative approach. J Am Coll Cardiol. 2016;68:2412–2421. - PubMed
-
- American Heart Association . Cardiovascular disease: A costly burden for America. Cost projections through 2035. 2017. Available at: http://www.heart.org/idc/groups/heart-public/@wcm/@adv/documents/downloa.... Accessed January 10, 2018.
-
- Nordestgaard BG. Triglyceride‐rich lipoproteins and atherosclerotic cardiovascular disease. New Insights From epidemiology, genetics, and biology. Circ Res. 2016;118:547–563. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
