

Statins Reduce Abdominal Aortic Aneurysm Growth, Rupture, and Perioperative Mortality: A Systematic Review and Meta-Analysis
- PMID: 30371297
- PMCID: PMC6404894
- DOI: 10.1161/JAHA.118.008657
Statins Reduce Abdominal Aortic Aneurysm Growth, Rupture, and Perioperative Mortality: A Systematic Review and Meta-Analysis
Abstract
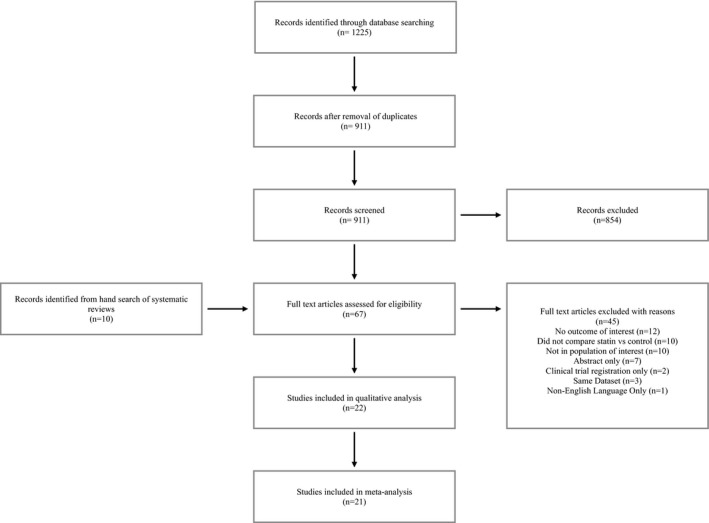
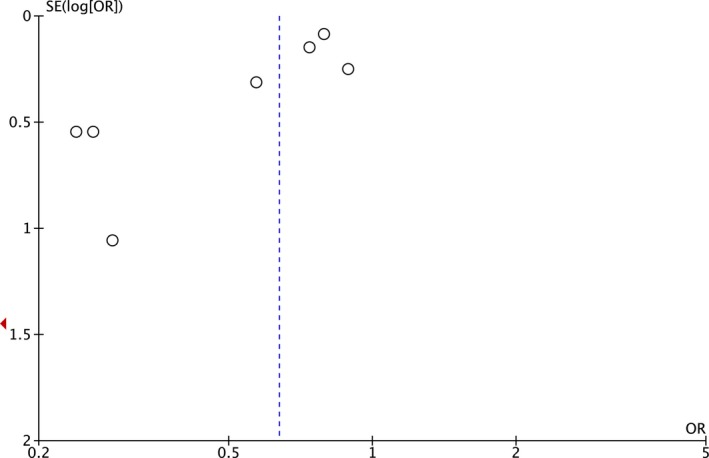
Background There are no recognized pharmacological treatments for abdominal aortic aneurysms ( AAA ), although statins are suggested to be beneficial. We sought to summarize the literature regarding the effects of statins on human AAA growth, rupture, and 30-day mortality. Methods and Results We conducted a systematic review and meta-analysis of randomized and observational studies using the Cochrane CENTRAL database, MEDLINE , and EMBASE up to June 15, 2018. Review, abstraction, and quality assessment were conducted by 2 independent reviewers, and a third author resolved discrepancies. Pooled mean differences and odds ratios with 95% confidence intervals were calculated using random effects models. Heterogeneity was quantified using the I2 statistic, and publication bias was assessed using funnel plots. Our search yielded 911 articles. One case-control and 21 cohort studies involving 80 428 patients were included. The risk of bias was low to moderate. Statin use was associated with a mean AAA growth rate reduction of 0.82 mm/y (95% confidence interval 0.33, 1.32, P=0.001, I2=86%). Statins were also associated with a lower rupture risk (odds ratio 0.63, 95% confidence interval 0.51, 0.78, P<0.0001, I2=27%), and preoperative statin use was associated with a lower 30-day mortality following elective AAA repair (odds ratio 0.55, 95% confidence interval 0.36, 0.83, P=0.005, I2=57%). Conclusions Statin therapy may be associated with reduction in AAA progression, rupture, and lower rates of perioperative mortality following elective AAA repair. These data argue for widespread statin use in AAA patients. Clinical Trial Registration URL : www.crd.york.ac.uk . Unique identifier: CRD 42017056480.
Keywords: aneurysm; meta‐analysis; rupture; statin; systematic review.
Figures









References
-
- Powell JT, Sweeting MJ, Brown LC, Gotensparre SM, Fowkes FG, Thompson SG. Systematic review and meta‐analysis of growth rates of small abdominal aortic aneurysms. Br J Surg. 2011;98:609–618. - PubMed
-
- Schermerhorn ML, O'Malley AJ, Jhaveri A, Cotterill P, Pomposelli F, Landon BE. Endovascular vs. open repair of abdominal aortic aneurysms in the Medicare population. N Engl J Med. 2008;358:464–474. - PubMed
-
- Lee WA, Carter JW, Upchurch G, Seeger JM, Huber TS. Perioperative outcomes after open and endovascular repair of intact abdominal aortic aneurysms in the United States during 2001. J Vasc Surg. 2004;39:491–496. - PubMed
-
- Lifeline Registry of EPC . Lifeline registry of endovascular aneurysm repair: long‐term primary outcome measures. J Vasc Surg. 2005;42:1–10. - PubMed
-
- van Marrewijk CJ, Leurs LJ, Vallabhaneni SR, Harris PL, Buth J, Laheij RJ; EUROSTAR Collaborators . Risk‐adjusted outcome analysis of endovascular abdominal aortic aneurysm repair in a large population: how do stent‐grafts compare? J Endovasc Ther. 2005;12:417–429. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
