

Fifteen-Year Trends in Management and Outcomes of Non-ST-Segment-Elevation Myocardial Infarction Among Black and White Patients: The ARIC Community Surveillance Study, 2000-2014
- PMID: 30371336
- PMCID: PMC6404893
- DOI: 10.1161/JAHA.118.010203
Fifteen-Year Trends in Management and Outcomes of Non-ST-Segment-Elevation Myocardial Infarction Among Black and White Patients: The ARIC Community Surveillance Study, 2000-2014
Abstract
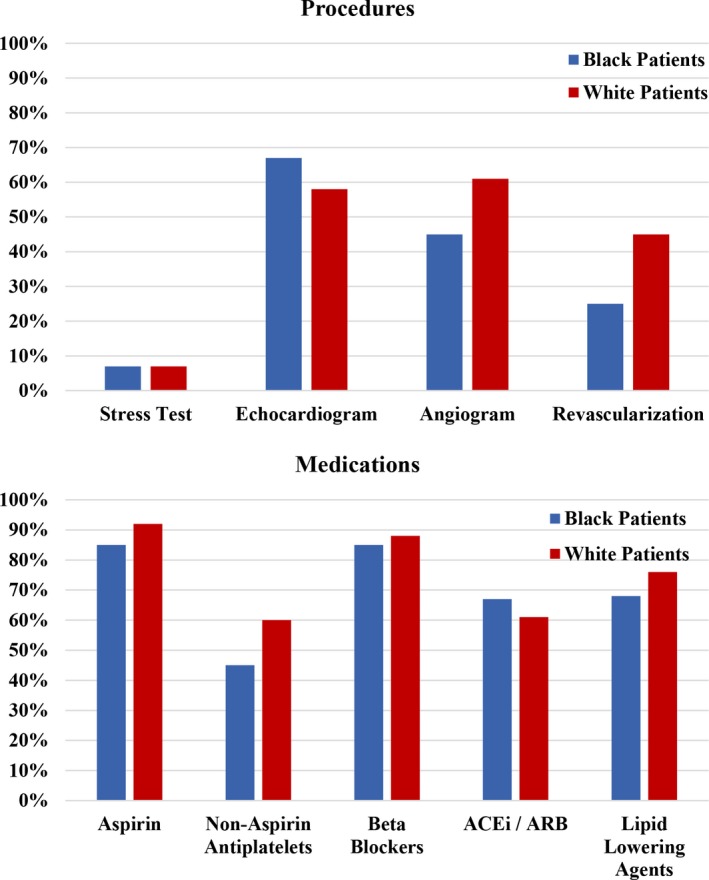
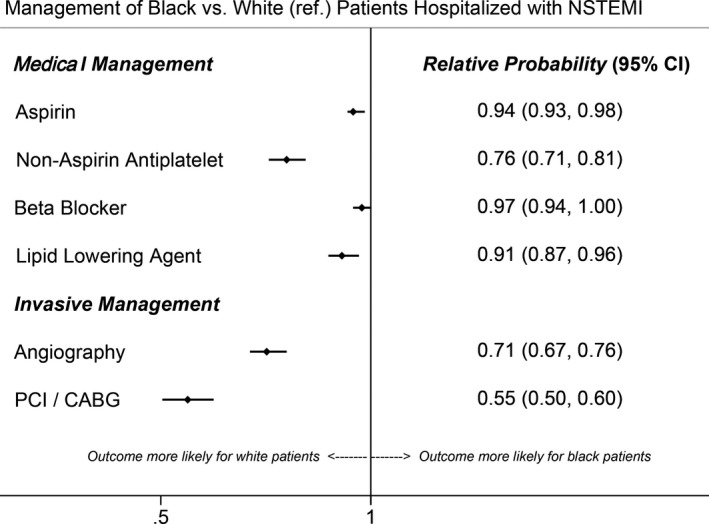
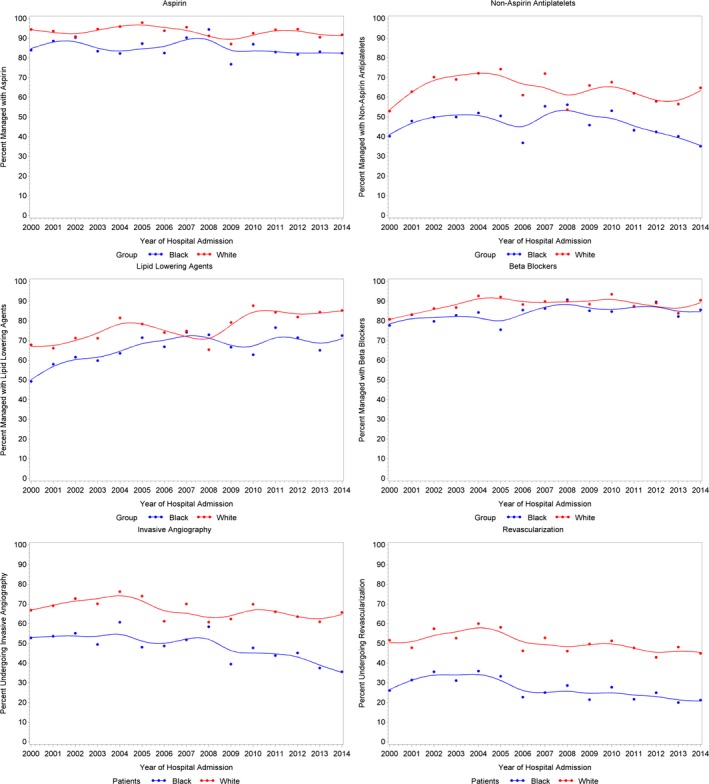
Background Standardization of evidence-based medical therapies has improved outcomes for patients with non- ST -segment-elevation myocardial infarction ( NSTEMI ). Although racial differences in NSTEMI management have previously been reported, it is uncertain whether these differences have been ameliorated over time. Methods and Results The ARIC (Atherosclerosis Risk in Communities) Community Surveillance study conducts hospital surveillance of acute myocardial infarction in 4 US communities. NSTEMI was classified by physician review, using a validated algorithm. From 2000 to 2014, 17 755 weighted hospitalizations for NSTEMI (patient race: 36% black, 64% white) were sampled by ARIC . Black patients were younger (aged 60 versus 66 years), more often female (45% versus 38%), and less likely to have medical insurance (88% versus 93%) but had more comorbidities. Black patients were less often administered aspirin (85% versus 92%), other antiplatelet therapy (45% versus 60%), β-blockers (85% versus 88%), and lipid-lowering medications (68% versus 76%). After adjustments, black patients had a 24% lower probability of receiving nonaspirin antiplatelets (relative risk: 0.76; 95% confidence interval, 0.71-0.81), a 29% lower probability of angiography (relative risk: 0.71; 95% confidence interval, 0.67-0.76), and a 45% lower probability of revascularization (relative risk: 0.55; 95% confidence interval, 0.50-0.60). No suggestion of a changing trend over time was observed for any NSTEMI therapy ( P values for interaction, all >0.20). Conclusions This longitudinal community surveillance of hospitalized NSTEMI patients suggests black patients have more comorbidities and less likelihood of receiving guideline-based NSTEMI therapies, and these findings persisted across the 15-year period. Focused efforts to reduce comorbidity burden and to more consistently implement guideline-directed treatments in this high-risk population are warranted.
Keywords: guideline adherence; myocardial infarction; quality of care; race.
Figures
Similar articles
-
Race and Sex Differences in Management and Outcomes of Patients After ST-Elevation and Non-ST-Elevation Myocardial Infarct: Results From the NCDR.Clin Cardiol. 2016 Oct;39(10):585-595. doi: 10.1002/clc.22570. Epub 2016 Jul 28. Clin Cardiol. 2016. PMID: 27468142 Free PMC article.
-
Temporal trends in medical therapies for ST- and non-ST elevation myocardial infarction: (from the Atherosclerosis Risk in Communities [ARIC] Surveillance Study).Am J Cardiol. 2013 Feb 1;111(3):305-11. doi: 10.1016/j.amjcard.2012.09.032. Epub 2012 Nov 17. Am J Cardiol. 2013. PMID: 23168284 Free PMC article.
-
Twenty Year Trends and Sex Differences in Young Adults Hospitalized With Acute Myocardial Infarction.Circulation. 2019 Feb 19;139(8):1047-1056. doi: 10.1161/CIRCULATIONAHA.118.037137. Circulation. 2019. PMID: 30586725 Free PMC article.
-
Contemporary NSTEMI management: the role of the hospitalist.Hosp Pract (1995). 2020 Feb;48(1):1-11. doi: 10.1080/21548331.2020.1701329. Epub 2020 Feb 20. Hosp Pract (1995). 2020. PMID: 31815570 Review.
-
Invasive and antiplatelet treatment of patients with non-ST-segment elevation myocardial infarction: Understanding and addressing the global risk-treatment paradox.Clin Cardiol. 2019 Oct;42(10):1028-1040. doi: 10.1002/clc.23232. Epub 2019 Jul 17. Clin Cardiol. 2019. PMID: 31317575 Free PMC article. Review.
Cited by
-
Gender, racial and ethnic disparities in acute coronary syndromes with coronary in-stent restenosis.Am Heart J Plus. 2024 May 20;43:100405. doi: 10.1016/j.ahjo.2024.100405. eCollection 2024 Jul. Am Heart J Plus. 2024. PMID: 38831788 Free PMC article.
-
2022 consensus conference on diversity, equity, and inclusion: Developing an emergency medicine research agenda for addressing racism through health care research.Acad Emerg Med. 2023 Jul;30(7):731-741. doi: 10.1111/acem.14742. Epub 2023 May 14. Acad Emerg Med. 2023. PMID: 37078910 Free PMC article.
-
Outcomes of decreasing versus increasing cardiac troponin in patients admitted with non-ST-segment elevation myocardial infarction: the Atherosclerosis Risk in Communities Surveillance Study.Eur Heart J Acute Cardiovasc Care. 2021 Dec 6;10(9):1048-1055. doi: 10.1177/2048872619842983. Eur Heart J Acute Cardiovasc Care. 2021. PMID: 30958029 Free PMC article.
-
Response by Arora et al to Letter Regarding Article, "Twenty Year Trends and Sex Differences in Young Adults Hospitalized With Acute Myocardial Infarction: The ARIC Community Surveillance Study".Circulation. 2019 Aug 20;140(8):e331-e332. doi: 10.1161/CIRCULATIONAHA.119.041483. Epub 2019 Aug 19. Circulation. 2019. PMID: 31424983 Free PMC article. No abstract available.
-
Racial Disparities in Cardiovascular Risk and Cardiovascular Care in Women.Curr Cardiol Rep. 2022 Sep;24(9):1197-1208. doi: 10.1007/s11886-022-01738-w. Epub 2022 Jul 8. Curr Cardiol Rep. 2022. PMID: 35802234 Review.
References
-
- Carnethon MR, Pu J, Howard G, Albert MA, Anderson CAM, Bertoni AG, Mujahid MS, Palaniappan L, Taylor HA Jr, Willis M, Yancy CW; American Heart Association Council on Epidemiology and Prevention; Council on Cardiovascular Disease in the Young; Council on Cardiovascular and Stroke Nursing; Council on Clinical Cardiology; Council on Functional Genomics and Translational Biology ; and Stroke Council. Cardiovascular Health in African Americans: a Scientific Statement from the American Heart Association. Circulation. 2017;136:e393–e423. - PubMed
-
- Benjamin EJ, Blaha MJ, Chiuve SE, Cushman M, Das SR, Deo R, de Ferranti SD, Floyd J, Fornage M, Gillespie C, Isasi CR, Jimenez MC, Jordan LC, Judd SE, Lackland D, Lichtman JH, Lisabeth L, Liu S, Longenecker CT, Mackey RH, Matsushita K, Mozaffarian D, Mussolino ME, Nasir K, Neumar RW, Palaniappan L, Pandey DK, Thiagarajan RR, Reeves MJ, Ritchey M, Rodriguez CJ, Roth GA, Rosamond WD, Sasson C, Towfighi A, Tsao CW, Turner MB, Virani SS, Voeks JH, Willey JZ, Wilkins JT, Wu JH, Alger HM, Wong SS, Muntner P; American Heart Association Statistics Committee and Stroke Statistics Subcommittee . Heart disease and stroke statistics‐2017 update: a report from the American Heart Association. Circulation. 2017;135:e146–e603. - PMC - PubMed
-
- Whittle J, Conigliaro J, Good CB, Lofgren RP. Racial differences in the use of invasive cardiovascular procedures in the Department of Veterans Affairs medical system. N Engl J Med. 1993;329:621–627. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
