

Prognostic Factors for Physical Functioning After Multidisciplinary Rehabilitation in Patients With Chronic Musculoskeletal Pain: A Systematic Review and Meta-Analysis
- PMID: 30371517
- PMCID: PMC6343958
- DOI: 10.1097/AJP.0000000000000669
Prognostic Factors for Physical Functioning After Multidisciplinary Rehabilitation in Patients With Chronic Musculoskeletal Pain: A Systematic Review and Meta-Analysis
Abstract
Objectives: This systematic review aimed to identify and evaluate prognostic factors for long-term (≥6 mo) physical functioning in patients with chronic musculoskeletal pain following multidisciplinary rehabilitation (MDR).
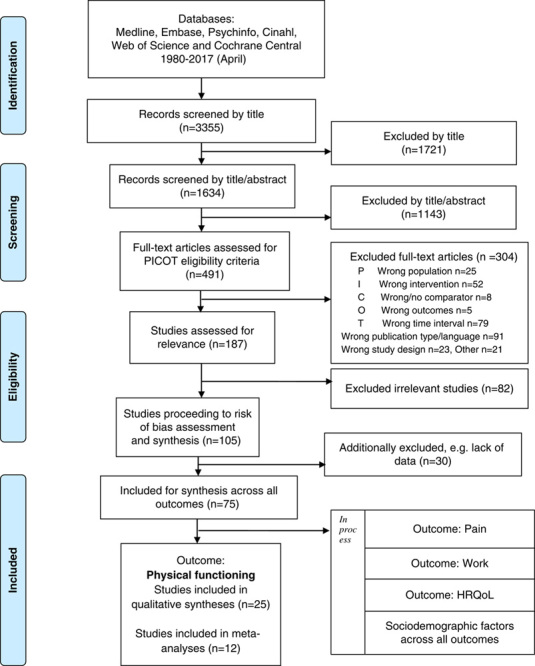
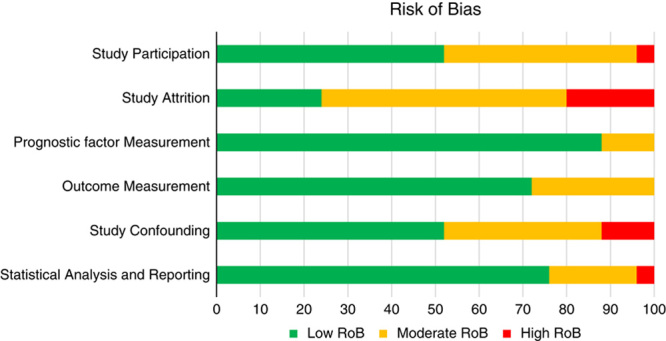
Materials and methods: Electronic searches conducted in MEDLINE, PsycINFO, EMBASE, CINAHL, Web of Science, and Cochrane CENTRAL revealed 25 original research reports, published 1983-2016, (n=9436). Potential prognostic factors relating to initial pain and physical and psychological functioning were synthesized qualitatively and quantitatively in random effects meta-analyses. The level of evidence (LoE) was evaluated with Grading of Recommendations Assessment, Development and Evaluation (GRADE).
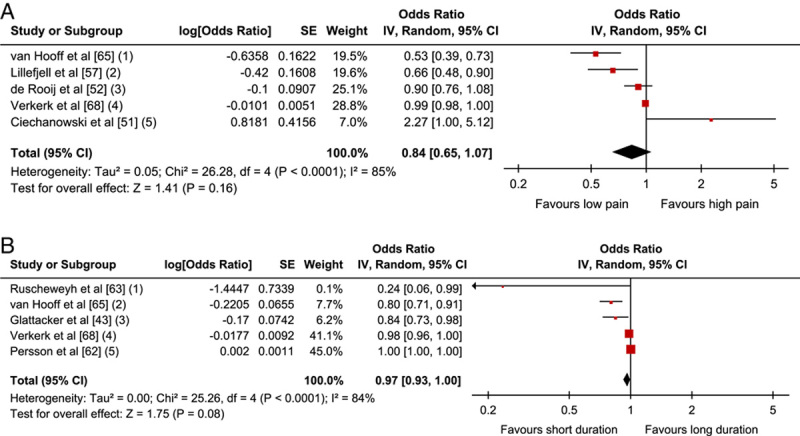
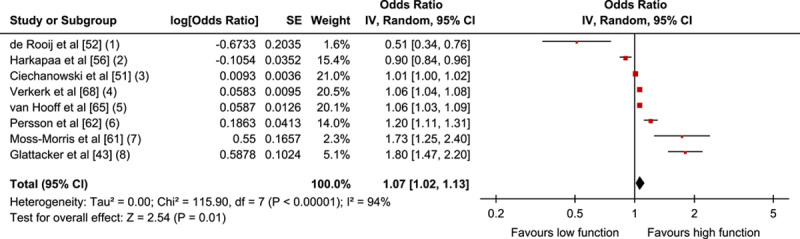
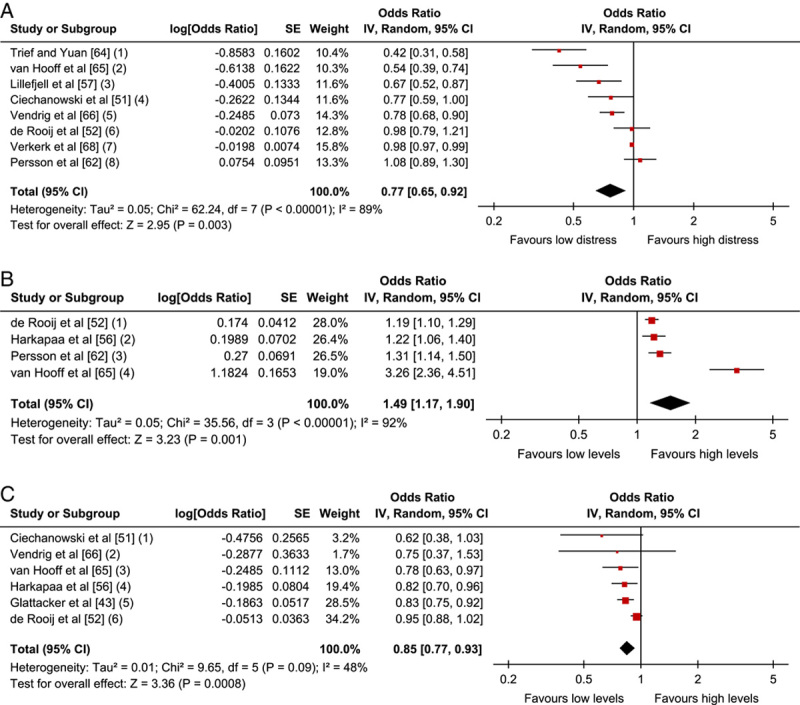
Results: Pain-related factors (intensity and chronicity) were not associated with function/disability at long-term follow-up, odds ratio (OR)=0.84; 95% confidence interval (CI), 0.65-1.07 and OR=0.97; 95% CI, 0.93-1.00, respectively (moderate LoE). A better function at follow-up was predicted by Physical factors; higher levels of initial self-reported functioning, OR=1.07; 95% CI, 1.02-1.13 (low LoE), and Psychological factors; low initial levels of emotional distress, OR=0.77; 95% CI, 0.65-0.92, low levels of cognitive and behavioral risk factors, OR=0.85; 95% CI, 0.77-0.93 and high levels of protective cognitive and behavioral factors, OR=1.49; 95% CI, 1.17-1.90 (moderate LoE).
Discussion: While pain intensity and long-term chronicity did not predict physical functioning in chronic pain patients after MDR, poor pretreatment physical and psychological functioning influenced the prognosis negatively. Thus, treatment should further target and optimize these modifiable factors and an increased focus on positive, psychological protective factors may perhaps provide an opening for yet untapped clinical gains.
Figures
References
-
- Taylor AM, Phillips K, Taylor JO, et al. Is chronic pain a disease in its own right? Discussions from a Pre-OMERACT 2014 Workshop on Chronic Pain. J Rheumatol. 2015;42:1947–1953. - PubMed
-
- Breivik H, Collett B, Ventafridda V, et al. Survey of chronic pain in Europe: prevalence, impact on daily life, and treatment. Eur J Pain. 2006;10:287–333. - PubMed
-
- Leadley RM, Armstrong N, Lee YC, et al. Chronic diseases in the European Union: the prevalence and health cost implications of chronic pain. J Pain Palliat Care Pharmacother. 2012;26:310–325. - PubMed
-
- Turk DC, Dworkin RH, Revicki D, et al. Identifying important outcome domains for chronic pain clinical trials: an IMMPACT survey of people with pain. Pain. 2008;137:276–285. - PubMed
-
- International Association for the Study of Pain. Task force on multimodal pain treatment defines terms for chronic pain care. 2017. Available at: www.iasp-pain.org/PublicationsNews/NewsDetail.aspx?ItemNumber=6981. Accessed December 14, 2017.
