

Comparison of Noninvasive Dynamic Indices of Fluid Responsiveness Among Different Ventilation Modes in Dogs Recovering from Experimental Cardiac Surgery
- PMID: 30372425
- PMCID: PMC6216474
- DOI: 10.12659/MSM.910135
Comparison of Noninvasive Dynamic Indices of Fluid Responsiveness Among Different Ventilation Modes in Dogs Recovering from Experimental Cardiac Surgery
Abstract
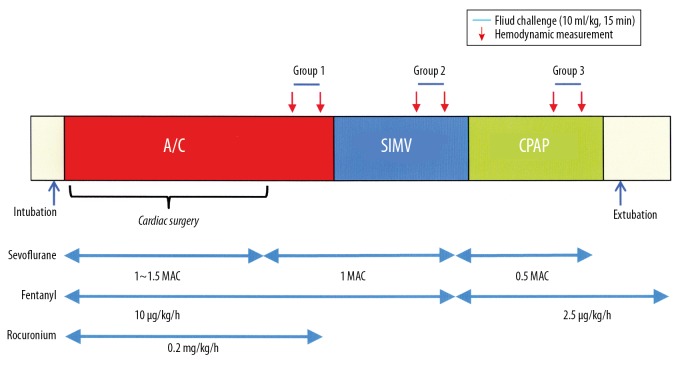
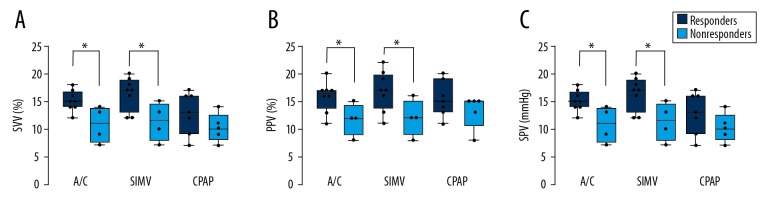
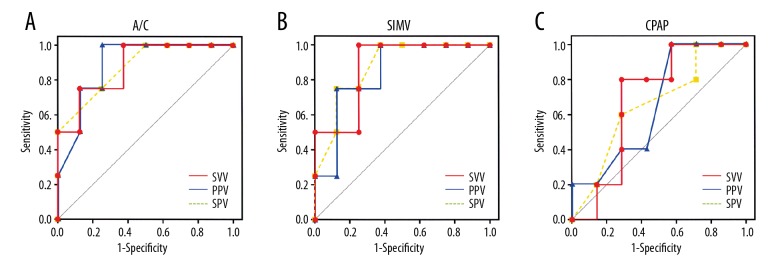
BACKGROUND Fluid resuscitation is a cornerstone of minimizing morbidity and mortality in critically ill patients, but the techniques for predicting fluid responsiveness is still a matter of debate. In this study, we aimed to evaluate the utility of noninvasive stroke volume variation (SVV), pulse pressure variation (PPV), and systolic pressure variation (SPV) as a dynamic predictor for assessing fluid responsiveness during different ventilation modes in anaesthetized, intubated dogs recovering from cardiac surgery. MATERIAL AND METHODS Thirty-six adult Beagle dogs undergoing experimental surgery for isolated right ventricular failure were monitored for SVV, PPV, and SPV simultaneously using electrical velocimetry device. The relationships between each indicator and SVI before and after volume loading were compared in 3 ventilatory modes: assist control (A/C), synchronized intermittent mandatory ventilation (SIMV), and continuous positive airway pressure (CPAP). Responders were defined as those whose stroke volume index increased by ≥10%. RESULTS In all of the indices, the baseline values were greater in responders than in nonresponders (P<0.01) under A/C and SIMV. Receiver operating curve analysis confirmed the best predictive value during A/C [area under the curve (AUC): SVV, 0.90; PPV, 0.88; SPV, 0.85; P<0.05] followed by SIMV (AUC: SVV, 0.86; PPV, 0.83; CPAP, 0.80; P<0.05), with their sensitivities and specificities of ≥7 5%. By contrast, no statistically significance detected in any parameter during CPAP (AUC: SVV, 0.71; PPV, 0.66; CPAP, 0.65; P>0.05). CONCLUSIONS SVV, PPV, and SVV are all useful to predict cardiac response to fluid loading in dogs during A/C and SIMV, while their reliabilities during CPAP are poor.
Conflict of interest statement
None.
Figures
Similar articles
-
[Stroke volume and pulse pressure variation are good predictors of fluid responsiveness in sepsis patients].Acta Med Croatica. 2013 Dec;67(5):407-14. Acta Med Croatica. 2013. PMID: 24979881 Croatian.
-
Noninvasive stroke volume variation using electrical velocimetry for predicting fluid responsiveness in dogs undergoing cardiac surgery.Vet Anaesth Analg. 2017 Jul;44(4):719-726. doi: 10.1016/j.vaa.2016.11.001. Epub 2017 Jan 11. Vet Anaesth Analg. 2017. PMID: 28803717
-
Utility of electrical velocimetry-based noninvasive stroke volume variation in predicting fluid responsiveness under different ventilation modes in anaesthetized dogs.Clin Exp Pharmacol Physiol. 2018 May 16. doi: 10.1111/1440-1681.12968. Online ahead of print. Clin Exp Pharmacol Physiol. 2018. PMID: 29767416
-
Reliability of pulse pressure and stroke volume variation in assessing fluid responsiveness in the operating room: a metanalysis and a metaregression.Crit Care. 2023 Nov 8;27(1):431. doi: 10.1186/s13054-023-04706-0. Crit Care. 2023. PMID: 37940953 Free PMC article.
-
Fluid Challenge During Anesthesia: A Systematic Review and Meta-analysis.Anesth Analg. 2018 Dec;127(6):1353-1364. doi: 10.1213/ANE.0000000000003834. Anesth Analg. 2018. PMID: 30300177
Cited by
-
Interventional Heartworm Extraction in Two Dogs: The Clinical Application of Impedance Cardiography.Animals (Basel). 2023 Oct 7;13(19):3127. doi: 10.3390/ani13193127. Animals (Basel). 2023. PMID: 37835733 Free PMC article.
-
Noninvasive assessment of fluid responsiveness for emergency abdominal surgery in dogs with pulmonary hypertension: Insights into high-risk companion animal anesthesia.PLoS One. 2020 Oct 23;15(10):e0241234. doi: 10.1371/journal.pone.0241234. eCollection 2020. PLoS One. 2020. PMID: 33095826 Free PMC article.
-
Evaluation of the caudal vena cava diameter to abdominal aortic diameter ratio and the caudal vena cava respiratory collapsibility for predicting fluid responsiveness in a heterogeneous population of hospitalized conscious dogs.J Vet Med Sci. 2020 Mar 24;82(3):337-344. doi: 10.1292/jvms.19-0028. Epub 2020 Jan 13. J Vet Med Sci. 2020. PMID: 31932519 Free PMC article.
-
Real-Time Monitoring of Cardiac Output Using Non-Invasive Impedance Cardiography in Dogs: A Pilot Study on Heartworm Extraction and Gastric Decompression.Vet Sci. 2025 May 15;12(5):478. doi: 10.3390/vetsci12050478. Vet Sci. 2025. PMID: 40431571 Free PMC article.
References
-
- Kumar A, Anel R, Bunnell E, et al. Pulmonary artery occlusion pressure and central venous pressure fail to predict ventricular filling volume, cardiac performance, or the response to volume infusion in normal subjects. Crit Care Med. 2004;32:691–99. - PubMed
-
- Mutoh T, Kazumata K, Ajiki M, et al. Goal-directed fluid management by bedside transpulmonary hemodynamic monitoring after subarachnoid hemorrhage. Stroke. 2007;38:3218–24. - PubMed
-
- Mutoh T, Kazumata K, Ishikawa T, et al. Performance of bedside transpulmonary thermodilution monitoring for goal-directed hemodynamic management after subarachnoid hemorrhage. Stroke. 2009;40:2368–74. - PubMed
-
- Renner J, Gruenewald M, Quaden R, et al. Influence of increased intra-abdominal pressure on fluid responsiveness predicted by pulse pressure variation and stroke volume variation in a porcine model. Crit Care Med. 2009;37:650–58. - PubMed
-
- Renner J, Cavus E, Meybohm P, et al. Pulse pressure variation and stroke volume variation during different loading conditions in a paediatric animal model. Acta Anaesthesiol Scand. 2008;52:374–80. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
