

Comparison of Noninvasive Dynamic Indices of Fluid Responsiveness Among Different Ventilation Modes in Dogs Recovering from Experimental Cardiac Surgery
- PMID: 30372425
- PMCID: PMC6216474
- DOI: 10.12659/MSM.910135
Comparison of Noninvasive Dynamic Indices of Fluid Responsiveness Among Different Ventilation Modes in Dogs Recovering from Experimental Cardiac Surgery
Abstract
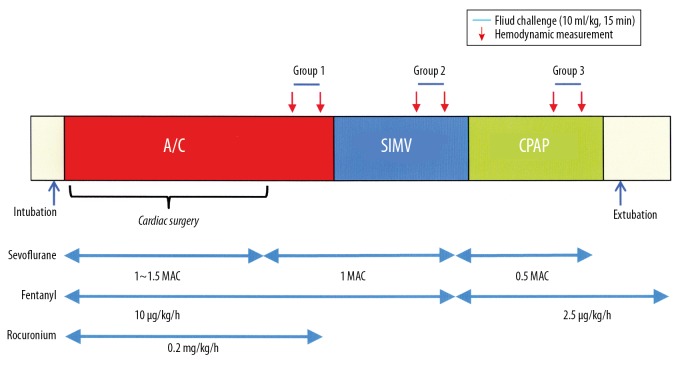
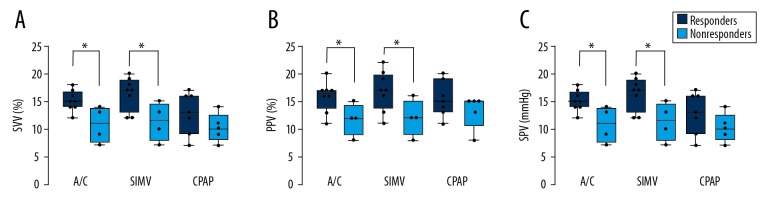
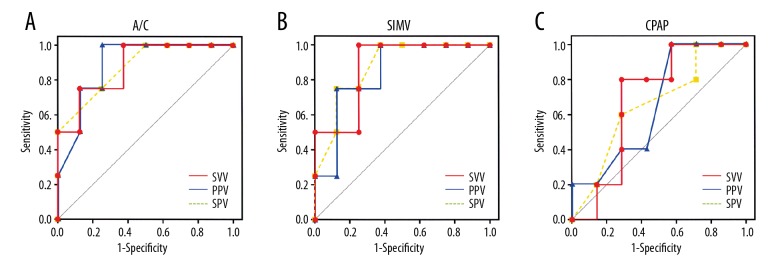
BACKGROUND Fluid resuscitation is a cornerstone of minimizing morbidity and mortality in critically ill patients, but the techniques for predicting fluid responsiveness is still a matter of debate. In this study, we aimed to evaluate the utility of noninvasive stroke volume variation (SVV), pulse pressure variation (PPV), and systolic pressure variation (SPV) as a dynamic predictor for assessing fluid responsiveness during different ventilation modes in anaesthetized, intubated dogs recovering from cardiac surgery. MATERIAL AND METHODS Thirty-six adult Beagle dogs undergoing experimental surgery for isolated right ventricular failure were monitored for SVV, PPV, and SPV simultaneously using electrical velocimetry device. The relationships between each indicator and SVI before and after volume loading were compared in 3 ventilatory modes: assist control (A/C), synchronized intermittent mandatory ventilation (SIMV), and continuous positive airway pressure (CPAP). Responders were defined as those whose stroke volume index increased by ≥10%. RESULTS In all of the indices, the baseline values were greater in responders than in nonresponders (P<0.01) under A/C and SIMV. Receiver operating curve analysis confirmed the best predictive value during A/C [area under the curve (AUC): SVV, 0.90; PPV, 0.88; SPV, 0.85; P<0.05] followed by SIMV (AUC: SVV, 0.86; PPV, 0.83; CPAP, 0.80; P<0.05), with their sensitivities and specificities of ≥7 5%. By contrast, no statistically significance detected in any parameter during CPAP (AUC: SVV, 0.71; PPV, 0.66; CPAP, 0.65; P>0.05). CONCLUSIONS SVV, PPV, and SVV are all useful to predict cardiac response to fluid loading in dogs during A/C and SIMV, while their reliabilities during CPAP are poor.
Conflict of interest statement
None.
Figures
References
-
- Kumar A, Anel R, Bunnell E, et al. Pulmonary artery occlusion pressure and central venous pressure fail to predict ventricular filling volume, cardiac performance, or the response to volume infusion in normal subjects. Crit Care Med. 2004;32:691–99. - PubMed
-
- Mutoh T, Kazumata K, Ajiki M, et al. Goal-directed fluid management by bedside transpulmonary hemodynamic monitoring after subarachnoid hemorrhage. Stroke. 2007;38:3218–24. - PubMed
-
- Mutoh T, Kazumata K, Ishikawa T, et al. Performance of bedside transpulmonary thermodilution monitoring for goal-directed hemodynamic management after subarachnoid hemorrhage. Stroke. 2009;40:2368–74. - PubMed
-
- Renner J, Gruenewald M, Quaden R, et al. Influence of increased intra-abdominal pressure on fluid responsiveness predicted by pulse pressure variation and stroke volume variation in a porcine model. Crit Care Med. 2009;37:650–58. - PubMed
-
- Renner J, Cavus E, Meybohm P, et al. Pulse pressure variation and stroke volume variation during different loading conditions in a paediatric animal model. Acta Anaesthesiol Scand. 2008;52:374–80. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
