

The national landscape of deceased donor kidney transplantation for the highly sensitized: Transplant rates, waitlist mortality, and posttransplant survival under KAS
- PMID: 30372592
- PMCID: PMC6433516
- DOI: 10.1111/ajt.15149
The national landscape of deceased donor kidney transplantation for the highly sensitized: Transplant rates, waitlist mortality, and posttransplant survival under KAS
Abstract
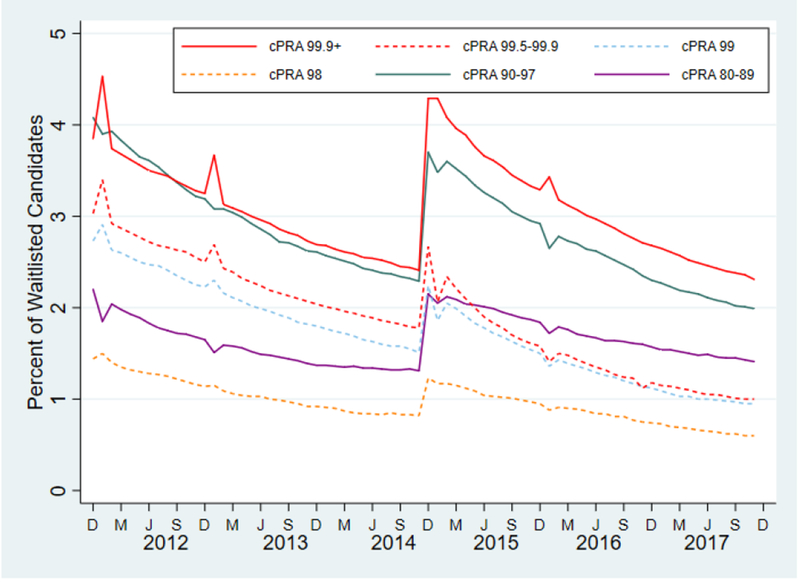
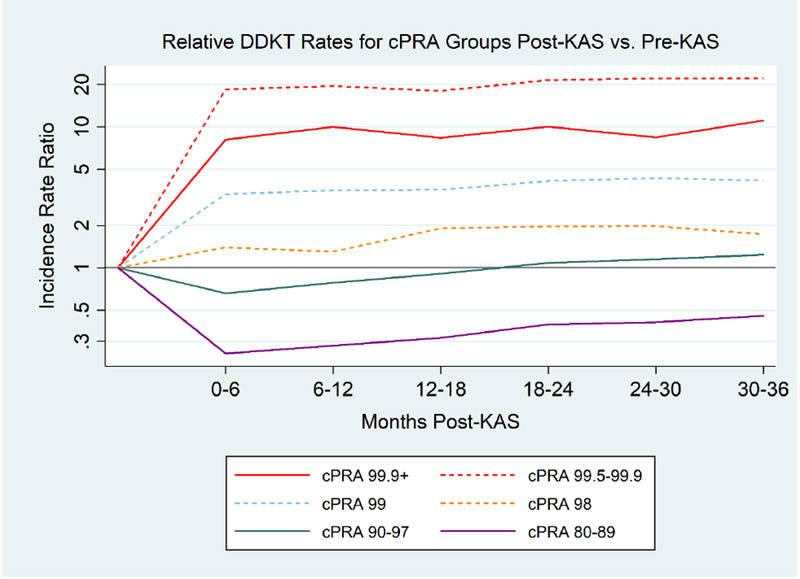
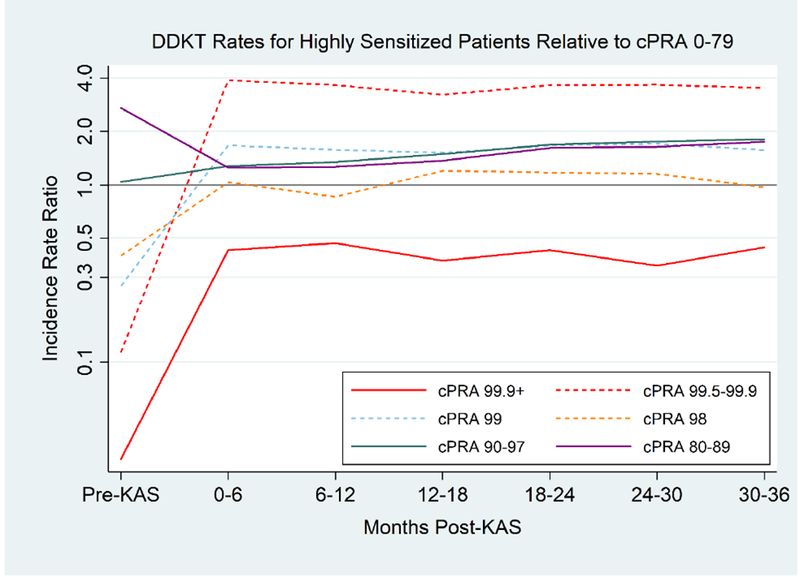
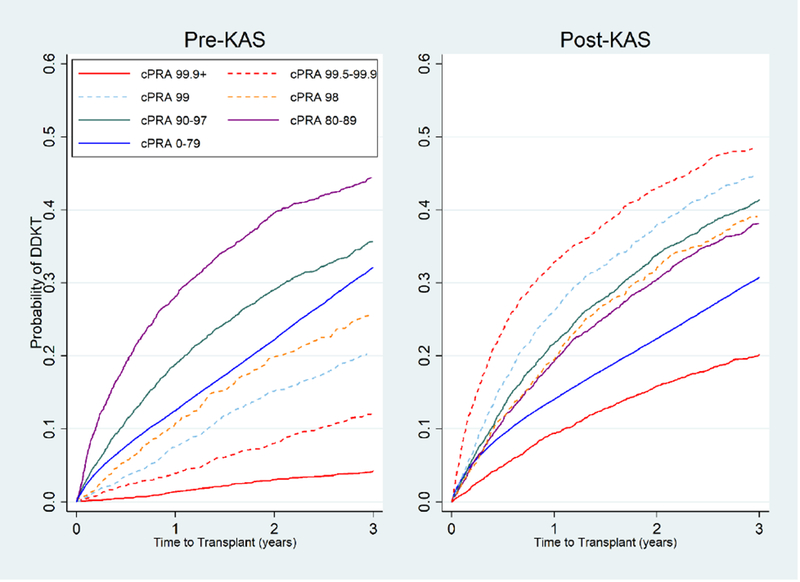
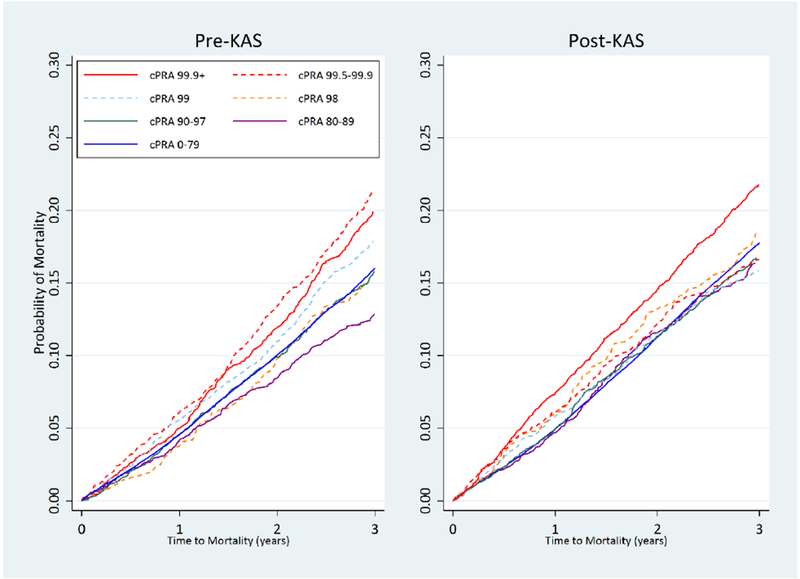
Deceased donor kidney transplantation (DDKT) rates for highly sensitized (HS) candidates increased early after implementation of the Kidney Allocation System (KAS) in 2014. However, this may represent a bolus effect, and a granular investigation of the current state of DDKT for HS candidates remains lacking. We studied 270 722 DDKT candidates from the SRTR from 12/4/2011 to 12/3/2014 ("pre-KAS") and 12/4/2014 to 12/3/2017 ("post-KAS"), analyzing DDKT rates for HS candidates using adjusted negative binomial regression. Post-KAS, candidates with the highest levels of sensitization had an increased DDKT rate compared with pre-KAS (cPRA 98% adjusted incidence rate ratio [aIRR]:1.27 1.772.46 P = .001, cPRA 99% aIRR:3.18 4.365.98 P < .001, cPRA 99.5-99.9% aIRR:16.91 24.2934.89 P < .001, and cPRA 99.9%+ aIRR:8.79 11.5815.26 P < .001). To determine whether these changes produced more equitable access to DDKT, we compared DDKT rates of HS to non-HS candidates (cPRA 0-79%). Post-KAS, cPRA, 98% candidates had an equivalent DDKT rate (aIRR:0.65 0.941.36 , P = .8) to non-HS candidates, whereas 99% candidates had a higher DDKT rate (aIRR:1.19 1.682.38 , P = .02). Although cPRA 99.5-99.9% candidates had an increased DDKT rate (aIRR:2.46 3.504.98 , P < .001) compared to non-HS candidates, cPRA 99.9%+ candidates had a significantly lower DDKT rate (aIRR:0.29 0.400.56 , P < .001). KAS has improved access to DDKT for HS candidates, although substantial imbalance exists between cPRA 99.5-99.9% and 99.9%+ candidates.
Keywords: clinical research/practice; health services and outcomes research; kidney transplantation/nephrology; organ allocation; organ procurement and allocation; panel-reactive antibody (PRA); sensitization.
© 2018 The American Society of Transplantation and the American Society of Transplant Surgeons.
Conflict of interest statement
DISCLOSURE
The authors of this manuscript have no conflicts of interest to disclose as described by the
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
