

The Pathophysiology of Gestational Diabetes Mellitus
- PMID: 30373146
- PMCID: PMC6274679
- DOI: 10.3390/ijms19113342
The Pathophysiology of Gestational Diabetes Mellitus
Abstract
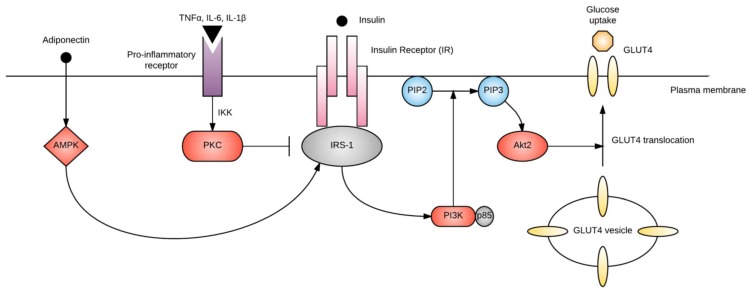
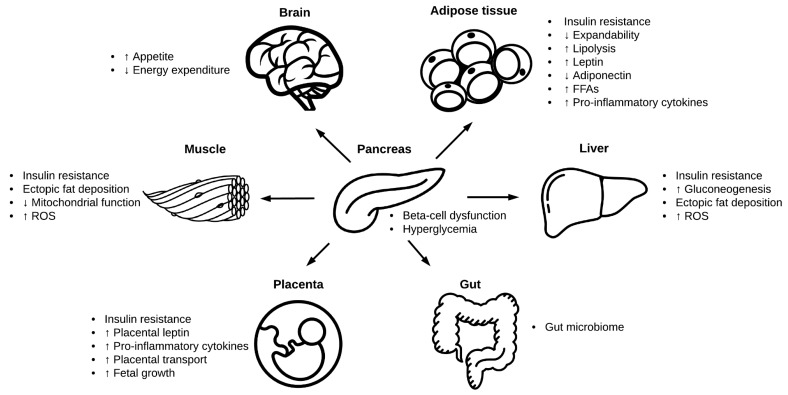
Gestational diabetes mellitus (GDM) is a serious pregnancy complication, in which women without previously diagnosed diabetes develop chronic hyperglycemia during gestation. In most cases, this hyperglycemia is the result of impaired glucose tolerance due to pancreatic β-cell dysfunction on a background of chronic insulin resistance. Risk factors for GDM include overweight and obesity, advanced maternal age, and a family history or any form of diabetes. Consequences of GDM include increased risk of maternal cardiovascular disease and type 2 diabetes and macrosomia and birth complications in the infant. There is also a longer-term risk of obesity, type 2 diabetes, and cardiovascular disease in the child. GDM affects approximately 16.5% of pregnancies worldwide, and this number is set to increase with the escalating obesity epidemic. While several management strategies exist-including insulin and lifestyle interventions-there is not yet a cure or an efficacious prevention strategy. One reason for this is that the molecular mechanisms underlying GDM are poorly defined. This review discusses what is known about the pathophysiology of GDM, and where there are gaps in the literature that warrant further exploration.
Keywords: gestational diabetes; molecular; pathology; pathophysiology; physiology; pregnancy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- International Diabetes Federation . IDF Diabetes Atlas. 8th ed. IDF; Brussels, Belgium: 2017.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
