

Left ventricular subclinical myocardial dysfunction in uncomplicated type 2 diabetes mellitus is associated with impaired myocardial perfusion: a contrast-enhanced cardiovascular magnetic resonance study
- PMID: 30373588
- PMCID: PMC6206833
- DOI: 10.1186/s12933-018-0782-0
Left ventricular subclinical myocardial dysfunction in uncomplicated type 2 diabetes mellitus is associated with impaired myocardial perfusion: a contrast-enhanced cardiovascular magnetic resonance study
Abstract
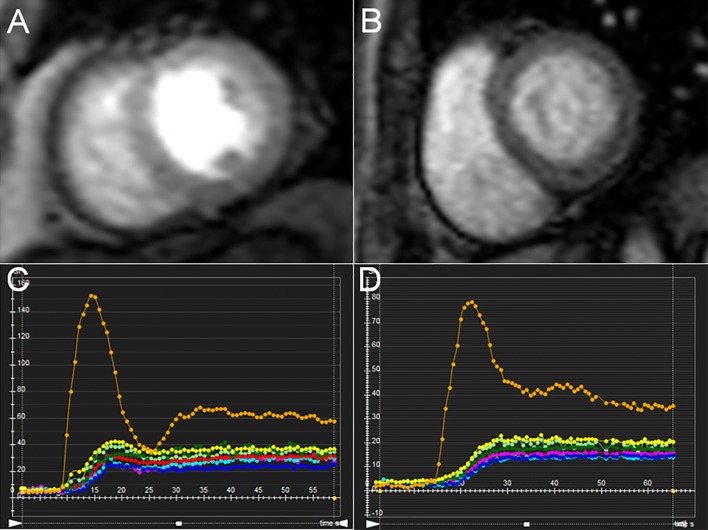
Background: Early detection of subclinical myocardial dysfunction in patients with diabetes mellitus (DM) is essential for recommending therapeutic interventions that can prevent or reverse heart failure, thereby improving the prognosis in such patients. This study aims to quantitatively evaluate left ventricular (LV) myocardial deformation and perfusion using cardiovascular magnetic resonance (CMR) imaging in patients with type 2 diabetes mellitus (T2DM), and to investigate the association between LV subclinical myocardial dysfunction and coronary microvascular perfusion.
Methods: We recruited 71 T2DM patients and 30 healthy individuals as controls who underwent CMR examination. The T2DM patients were subdivided into two groups, namely the newly diagnosed DM group (n = 31, patients with diabetes for ≤ 5 years) and longer-term DM group (n = 40, patients with diabetes > 5 years). LV deformation parameters, including global peak strain (PS), peak systolic strain rate, and peak diastolic strain rate (PSDR), and myocardial perfusion parameters such as upslope, time to maximum signal intensity (TTM), and max signal intensity (Max SI, were measured and compared among the three groups. Pearson's correlation was used to evaluate the correlation between LV deformation and perfusion parameters.
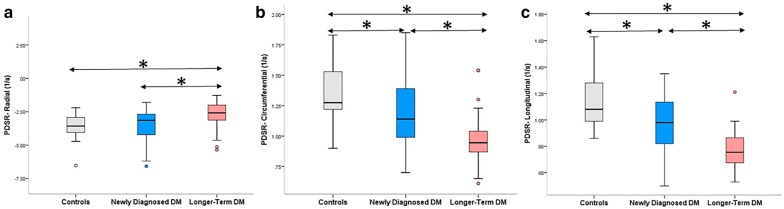
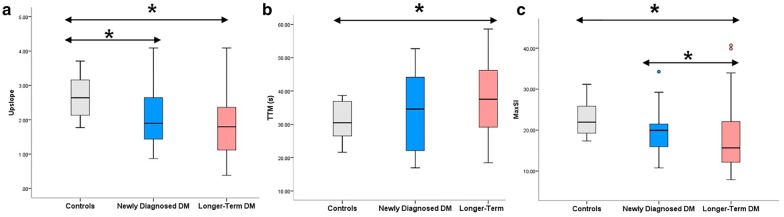
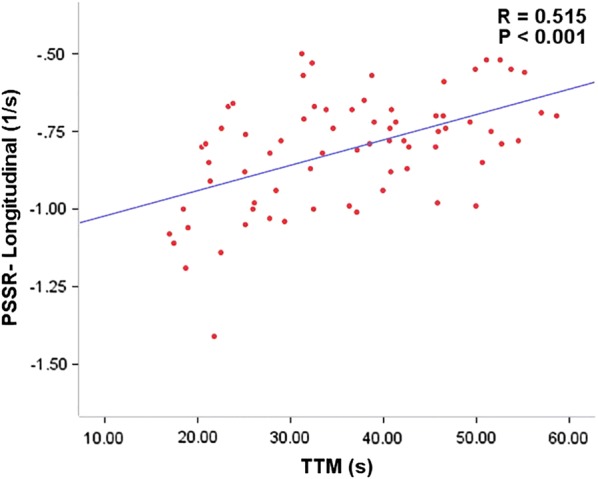
Results: Pooled data from T2DM patients showed a decrease in global longitudinal, circumferential, and radial PDSR compared to healthy individuals, apart from lower upslope. In addition, increased TTM and reduced Max SI were found in the longer-term diabetics compared to the normal subjects (p < 0.017 for all). Multivariable linear regression analysis showed that T2DM was independently associated with statistically significant CMR parameters, except for TTM (β = 0.137, p = 0.195). Further, longitudinal PDSR was significantly associated with upslope (r = - 0.346, p = 0.003) and TTM (r = 0.515, p < 0.001).
Conclusions: Our results imply that a contrast-enhanced 3.0T CMR can detect subclinical myocardial dysfunction and impaired myocardial microvascular perfusion in the early stages of T2DM, and that the myocardial dysfunction is associated with impaired coronary microvascular perfusion.
Keywords: Cardiac magnetic resonance; Myocardial perfusion; Subclinical myocardial dysfunction; Type 2 diabetes mellitus.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
- 81471721/National Natural Science Foundation of China/International
- 81471722/National Natural Science Foundation of China/International
- 81641169/National Natural Science Foundation of China/International
- 81771887/National Natural Science Foundation of China/International
- 81771897/National Natural Science Foundation of China/International
LinkOut - more resources
Full Text Sources
Medical
