

SwissMTB: establishing comprehensive molecular cancer diagnostics in Swiss clinics
- PMID: 30373609
- PMCID: PMC6206832
- DOI: 10.1186/s12911-018-0680-0
SwissMTB: establishing comprehensive molecular cancer diagnostics in Swiss clinics
Abstract
Background: Molecular precision oncology is an emerging practice to improve cancer therapy by decreasing the risk of choosing treatments that lack efficacy or cause adverse events. However, the challenges of integrating molecular profiling into routine clinical care are manifold. From a computational perspective these include the importance of a short analysis turnaround time, the interpretation of complex drug-gene and gene-gene interactions, and the necessity of standardized high-quality workflows. In addition, difficulties faced when integrating molecular diagnostics into clinical practice are ethical concerns, legal requirements, and limited availability of treatment options beyond standard of care as well as the overall lack of awareness of their existence.
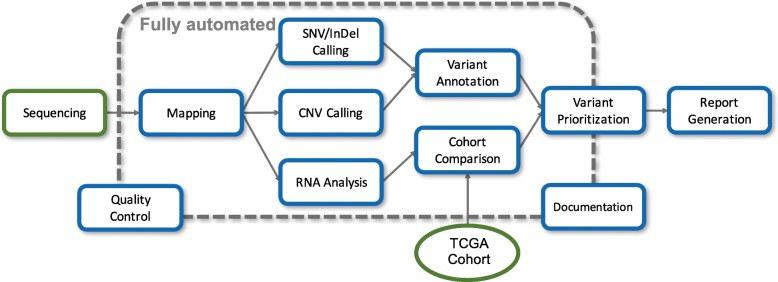
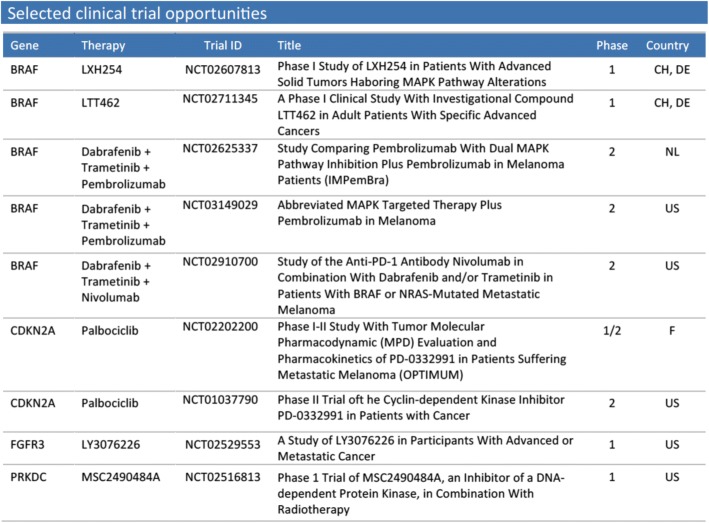
Methods: To the best of our knowledge, we are the first group in Switzerland that established a workflow for personalized diagnostics based on comprehensive high-throughput sequencing of tumors at the clinic. Our workflow, named SwissMTB (Swiss Molecular Tumor Board), links genetic tumor alterations and gene expression to therapeutic options and clinical trial opportunities. The resulting treatment recommendations are summarized in a clinical report and discussed in a molecular tumor board at the clinic to support therapy decisions.
Results: Here we present results from an observational pilot study including 22 late-stage cancer patients. In this study we were able to identify actionable variants and corresponding therapies for 19 patients. Half of the patients were analyzed retrospectively. In two patients we identified resistance-associated variants explaining lack of therapy response. For five out of eleven patients analyzed before treatment the SwissMTB diagnostic influenced treatment decision.
Conclusions: SwissMTB enables the analysis and clinical interpretation of large numbers of potentially actionable molecular targets. Thus, our workflow paves the way towards a more frequent use of comprehensive molecular diagnostics in Swiss hospitals.
Keywords: Cancer diagnostics; Molecular diagnostics; Molecular tumor board; NGS; Personalized medicine.
Conflict of interest statement
Ethics approval and consent to participate
All patients included in the observational pilot study gave informed written consent for research use of their tissue samples, based on the approved consent forms of the University Hospitals Zurich and Basel. In Zurich, surplus tumor material was obtained after surgical removal of melanoma metastases from patients after written informed consent approved by the local IRB (EK647 and EK800). In addition, a specific approval was given for this research project (KEK-ZH.2014–0425) by the Kantonal Ethics Commission of Zürich, Stampfenbachstrasse 121, Zürich Switzerland 8090, and the Ethical Committee of Northwestern and Central Part of Switzerland, EKNZ. The retrospective use of the pseudonymized data in Basel did not require written informed consent from individual patients. Pseudonymized clinical data only from patients that have signed a general consent statement of the University Hospital Basel were used for this study. Clinical data of patients from the University Hospital Basel were collected by SR and AW, staff members at the respective institution. All research on human patients followed the standards set by the Declaration of Helsinki on human rights, and the biobank samples were handled according to the international guidelines set by the Declaration of Taipei.
Consent for publication
Not applicable.
Competing interests
SIR: Research support: AbbVie, AstraZeneca, BMS, Merck; Honoraria for advisory boards (to the institution): Abbvie, AstraZeneca, BMS, Eisai, Merck, MSD, Novartis, Pfizer, Roche, Takeda.
DJS: Honoraria for scientific advisory board at BC Platforms.
All other authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


Similar articles
-
Implementation of a Molecular Tumor Board: The Impact on Treatment Decisions for 35 Patients Evaluated at Dartmouth-Hitchcock Medical Center.Oncologist. 2015 Sep;20(9):1011-8. doi: 10.1634/theoncologist.2015-0097. Epub 2015 Jul 23. Oncologist. 2015. PMID: 26205736 Free PMC article.
-
Real-world performance analysis of a novel computational method in the precision oncology of pediatric tumors.World J Pediatr. 2023 Oct;19(10):992-1008. doi: 10.1007/s12519-023-00700-2. Epub 2023 Mar 13. World J Pediatr. 2023. PMID: 36914906 Free PMC article.
-
Study protocol: Whole genome sequencing Implementation in standard Diagnostics for Every cancer patient (WIDE).BMC Med Genomics. 2020 Nov 10;13(1):169. doi: 10.1186/s12920-020-00814-w. BMC Med Genomics. 2020. PMID: 33167975 Free PMC article.
-
A 2015 update on predictive molecular pathology and its role in targeted cancer therapy: a review focussing on clinical relevance.Cancer Gene Ther. 2015 Sep;22(9):417-30. doi: 10.1038/cgt.2015.39. Epub 2015 Sep 11. Cancer Gene Ther. 2015. PMID: 26358176 Review.
-
Complexity of genome sequencing and reporting: Next generation sequencing (NGS) technologies and implementation of precision medicine in real life.Crit Rev Oncol Hematol. 2019 Jan;133:171-182. doi: 10.1016/j.critrevonc.2018.11.008. Epub 2018 Nov 26. Crit Rev Oncol Hematol. 2019. PMID: 30661654 Review.
Cited by
-
A showcase study on personalized in silico drug response prediction based on the genetic landscape of muscle invasive bladder cancer.Sci Rep. 2021 Mar 12;11(1):5849. doi: 10.1038/s41598-021-85151-3. Sci Rep. 2021. PMID: 33712636 Free PMC article.
-
scAmpi-A versatile pipeline for single-cell RNA-seq analysis from basics to clinics.PLoS Comput Biol. 2022 Jun 3;18(6):e1010097. doi: 10.1371/journal.pcbi.1010097. eCollection 2022 Jun. PLoS Comput Biol. 2022. PMID: 35658001 Free PMC article.
-
Variomes: a high recall search engine to support the curation of genomic variants.Bioinformatics. 2022 Apr 28;38(9):2595-2601. doi: 10.1093/bioinformatics/btac146. Bioinformatics. 2022. PMID: 35274687 Free PMC article.
-
Knowledge bases and software support for variant interpretation in precision oncology.Brief Bioinform. 2021 Nov 5;22(6):bbab134. doi: 10.1093/bib/bbab134. Brief Bioinform. 2021. PMID: 33971666 Free PMC article.
-
Development and validation of ACTE-MTB: A tool to systematically assess the maturity of molecular tumor boards.PLoS One. 2022 May 13;17(5):e0268477. doi: 10.1371/journal.pone.0268477. eCollection 2022. PLoS One. 2022. PMID: 35560035 Free PMC article.
References
-
- Hamblin A, Wordsworth S, Fermont JM, Page S, Kaur K, Camps C, et al. Clinical applicability and cost of a 46-gene panel for genomic analysis of solid tumours: retrospective validation and prospective audit in the UK National Health Service. PLoS Med. 2017;14:e1002230. doi: 10.1371/journal.pmed.1002230. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
