

Prospective Genotyping of Hepatocellular Carcinoma: Clinical Implications of Next-Generation Sequencing for Matching Patients to Targeted and Immune Therapies
- PMID: 30373752
- PMCID: PMC6689131
- DOI: 10.1158/1078-0432.CCR-18-2293
Prospective Genotyping of Hepatocellular Carcinoma: Clinical Implications of Next-Generation Sequencing for Matching Patients to Targeted and Immune Therapies
Abstract
Purpose: Prior molecular profiling of hepatocellular carcinoma (HCC) has identified actionable findings that may have a role in guiding therapeutic decision-making and clinical trial enrollment. We implemented prospective next-generation sequencing (NGS) in the clinic to determine whether such analyses provide predictive and/or prognostic information for HCC patients treated with contemporary systemic therapies.
Experimental design: Matched tumor/normal DNA from patients with HCC (N = 127) were analyzed using a hybridization capture-based NGS assay designed to target 341 or more cancer-associated genes. Demographic and treatment data were prospectively collected with the goal of correlating treatment outcomes and drug response with molecular profiles.
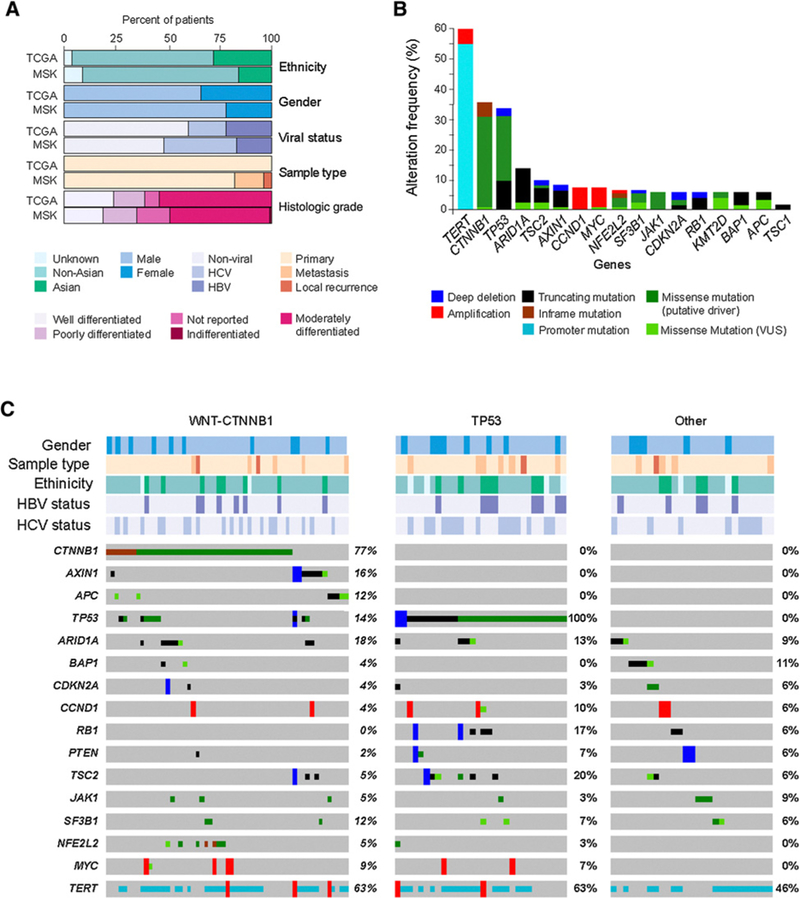
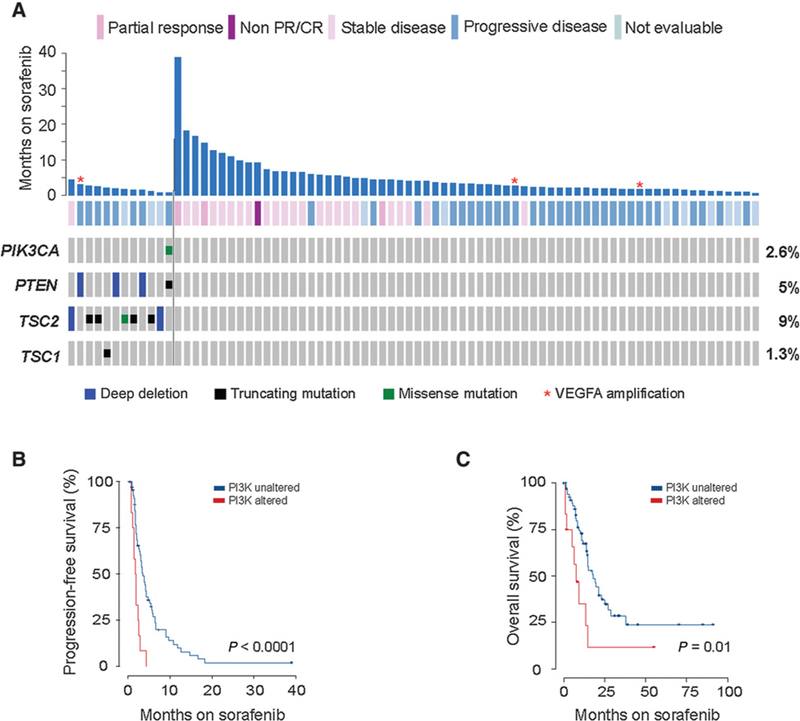
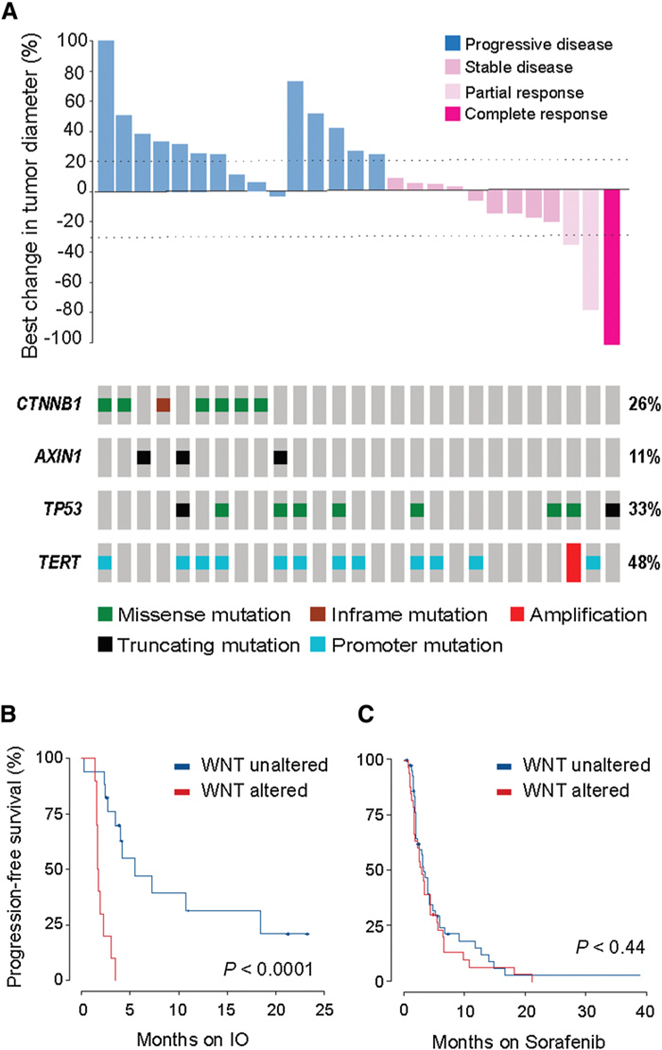
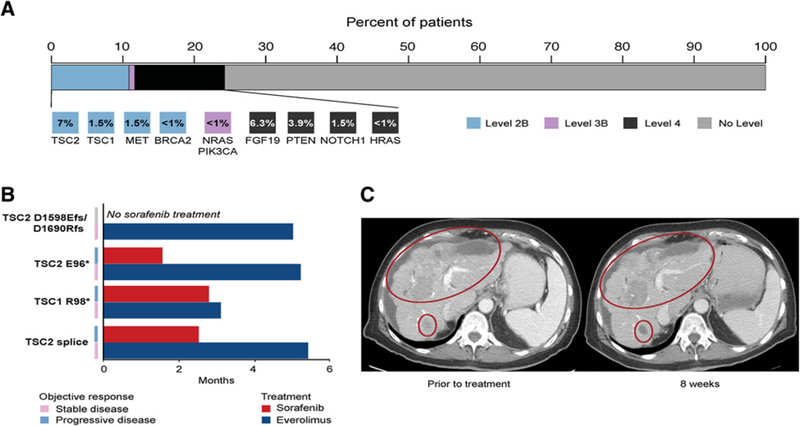
Results: WNT/β-catenin pathway (45%) and TP53 (33%) alterations were frequent and represented mutually exclusive molecular subsets. In sorafenib-treated patients (n = 81), oncogenic PI3K-mTOR pathway alterations were associated with lower disease control rates (DCR, 8.3% vs. 40.2%), shorter median progression-free survival (PFS; 1.9 vs. 5.3 months), and shorter median overall survival (OS; 10.4 vs. 17.9 months). For patients treated with immune checkpoint inhibitors (n = 31), activating alteration WNT/β-catenin signaling were associated with lower DCR (0% vs. 53%), shorter median PFS (2.0 vs. 7.4 months), and shorter median OS (9.1 vs. 15.2 months). Twenty-four percent of patients harbored potentially actionable alterations including TSC1/2 (8.5%) inactivating/truncating mutations, FGF19 (6.3%) and MET (1.5%) amplifications, and IDH1 missense mutations (<1%). Six percent of patients treated with systemic therapy were matched to targeted therapeutics.
Conclusions: Linking NGS to routine clinical care has the potential to identify those patients with HCC likely to benefit from standard systemic therapies and can be used in an investigational context to match patients to genome-directed targeted therapies.See related commentary by Pinyol et al., p. 2021.
©2018 American Association for Cancer Research.
Conflict of interest statement
Disclosure of Potential Conflicts of Interest
No potential conflicts of interest were disclosed by the other authors.
Figures
Comment in
-
Immune Exclusion-Wnt/CTNNB1 Class Predicts Resistance to Immunotherapies in HCC.Clin Cancer Res. 2019 Apr 1;25(7):2021-2023. doi: 10.1158/1078-0432.CCR-18-3778. Epub 2019 Jan 7. Clin Cancer Res. 2019. PMID: 30617138 Free PMC article.
References
-
- Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin 2015;65:87–108. - PubMed
-
- Llovet JM, Ricci S, Mazzaferro V, Hilgard P, Gane E, Blanc JF, et al. Sorafenib in advanced hepatocellular carcinoma. N Engl J Med 2008; 359:378–90. - PubMed
-
- Bruix J, Qin S, Merle P, Granito A, Huang YH, Bodoky G, et al. Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2016;389: 56–66. - PubMed
-
- Kudo M, Finn RS, Qin S, Han KH, Ikeda K, Piscaglia F, et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: a randomised phase 3 non-inferiority trial. Lancet 2018;391:1163–73. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
