Disease networks identify specific conditions and pleiotropy influencing multimorbidity in the general population
- PMID: 30374096
- PMCID: PMC6206057
- DOI: 10.1038/s41598-018-34361-3
Disease networks identify specific conditions and pleiotropy influencing multimorbidity in the general population
Abstract
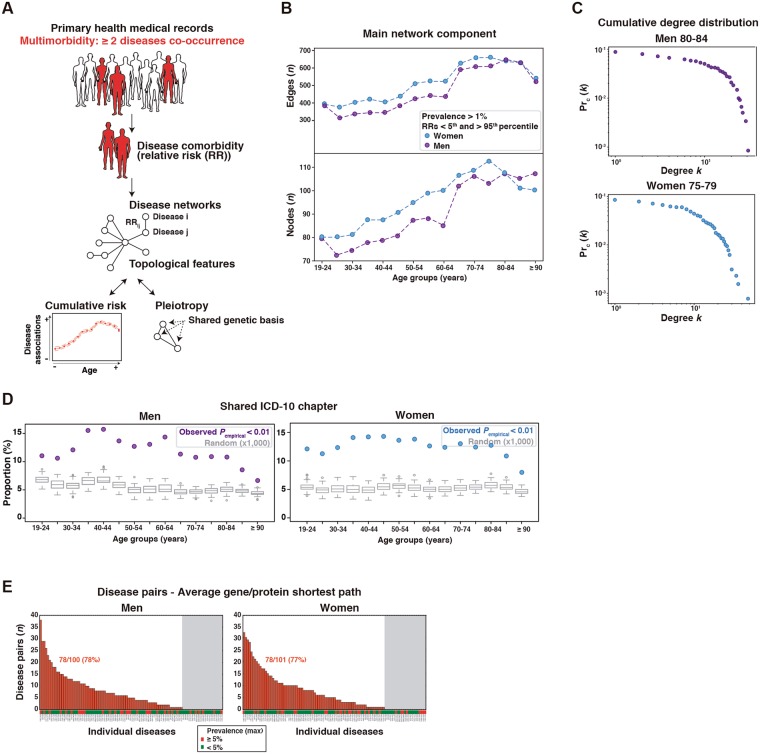
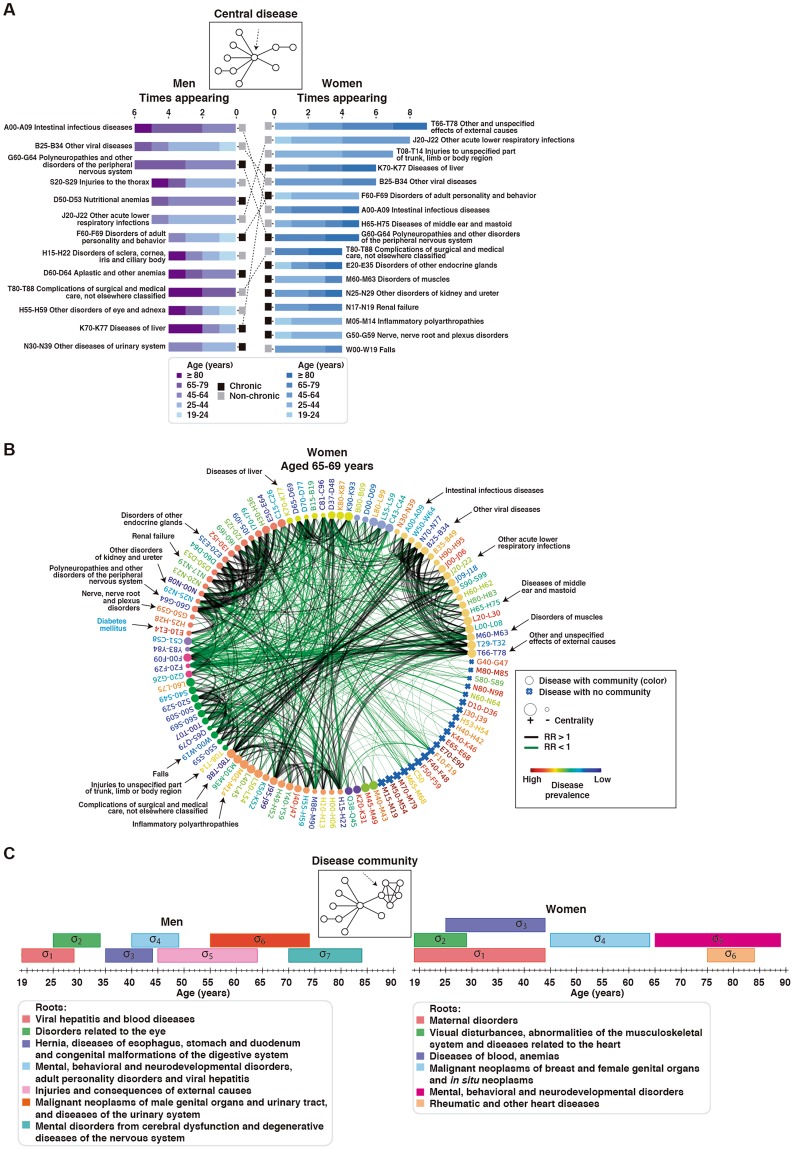
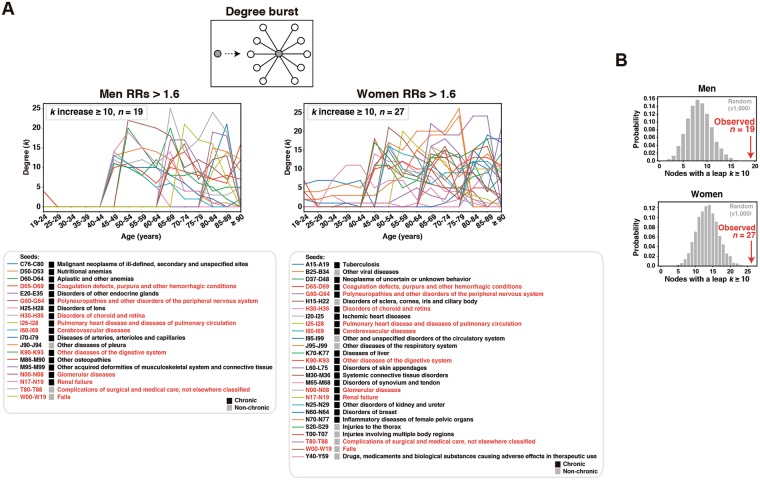
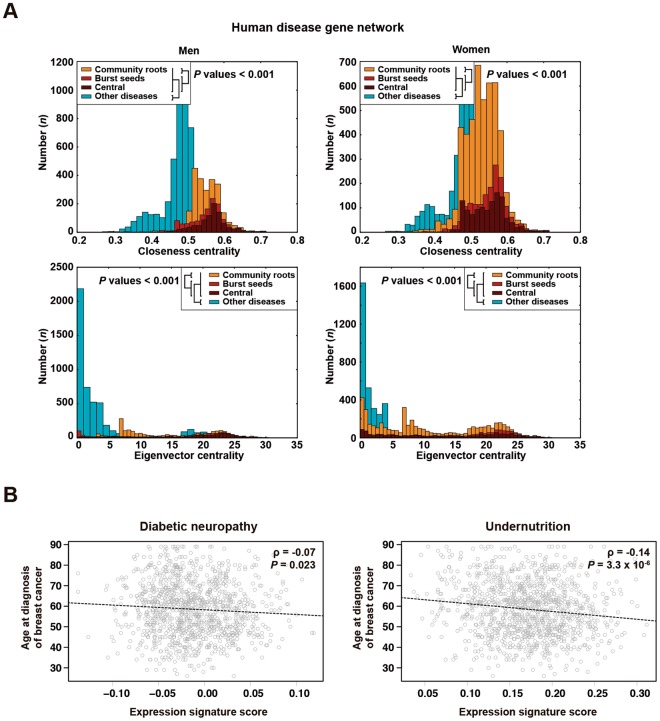
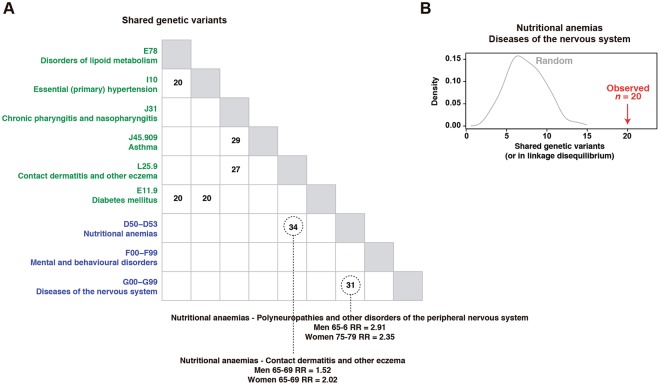
Multimorbidity is an emerging topic in public health policy because of its increasing prevalence and socio-economic impact. However, the age- and gender-dependent trends of disease associations at fine resolution, and the underlying genetic factors, remain incompletely understood. Here, by analyzing disease networks from electronic medical records of primary health care, we identify key conditions and shared genetic factors influencing multimorbidity. Three types of diseases are outlined: "central", which include chronic and non-chronic conditions, have higher cumulative risks of disease associations; "community roots" have lower cumulative risks, but inform on continuing clustered disease associations with age; and "seeds of bursts", which most are chronic, reveal outbreaks of disease associations leading to multimorbidity. The diseases with a major impact on multimorbidity are caused by genes that occupy central positions in the network of human disease genes. Alteration of lipid metabolism connects breast cancer, diabetic neuropathy and nutritional anemia. Evaluation of key disease associations by a genome-wide association study identifies shared genetic factors and further supports causal commonalities between nervous system diseases and nutritional anemias. This study also reveals many shared genetic signals with other diseases. Collectively, our results depict novel population-based multimorbidity patterns, identify key diseases within them, and highlight pleiotropy influencing multimorbidity.
Conflict of interest statement
M.A.P. is recipient of an unrestricted research grant from Roche Pharma for the support of the ProCURE research program of the Catalan Institute of Oncology.
Figures