

ADRB2 polymorphism Arg16Gly modifies the natural outcome of heart failure and dictates therapeutic response to β-blockers in patients with heart failure
- PMID: 30374408
- PMCID: PMC6198009
- DOI: 10.1038/s41421-018-0058-6
ADRB2 polymorphism Arg16Gly modifies the natural outcome of heart failure and dictates therapeutic response to β-blockers in patients with heart failure
Abstract
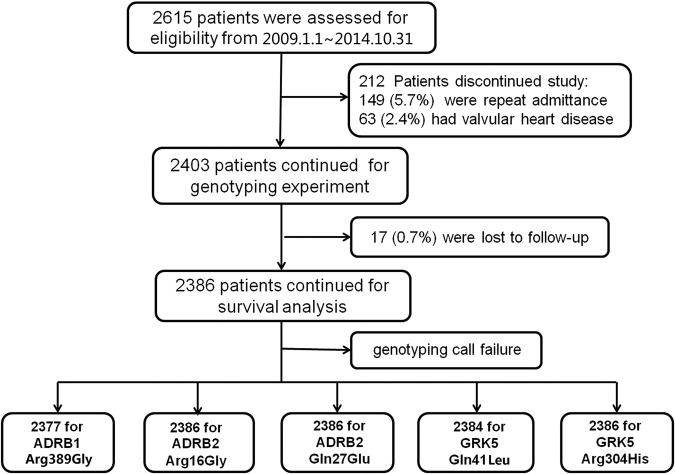
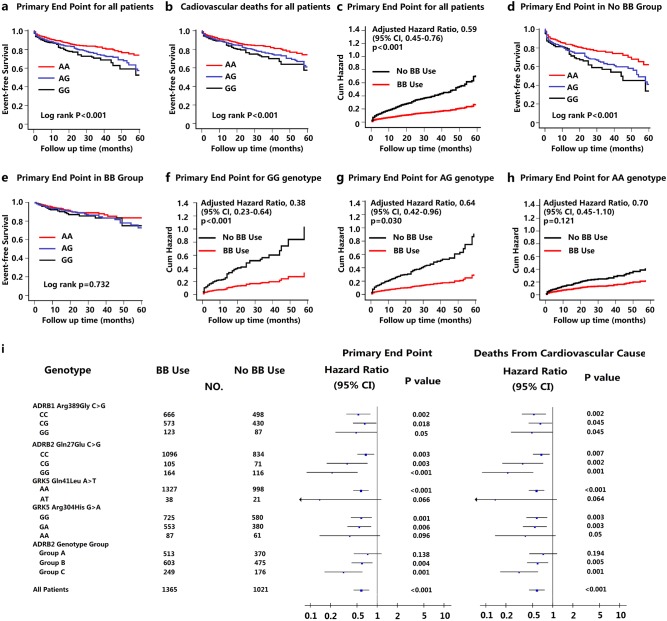
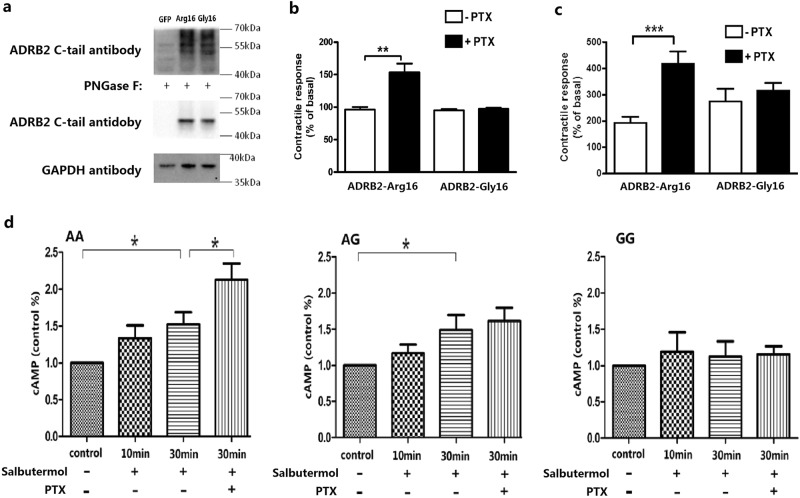
We sought to investigate the association of single nucleotide polymorphisms (SNPs) of the genes involved in βAR signaling with the response of patients to βAR blockers. A total of 2403 hospitalized patients with chronic heart failure (HF) were enrolled in a multicenter observational study as the first cohort and followed up for a mean period of 20 months. Genes for β1AR, β2AR, and the major cardiac G-protein-coupled receptor kinases (GRKs) GRK2 and GRK5 were analyzed to identify SNPs, and patients were stratified according to genotypes. A second independent cohort enrolling 919 patients with chronic HF was applied to validate the observed associations. The signaling properties of the key identified SNPs were assessed in vitro. Our data showed that HF patients harboring the Gly16 allele in the gene for β2AR (ADRB2) had an increased risk of the composite end point relative to patients who were homozygous for Arg16. Notably, these patients showed a beneficial response to βAR-blocker treatment in a G allele-dose-dependent manner, whereas Arg16 homozygotes had no response to βAR-blocker therapy. This Arg16Gly genotype-dependent heterogeneity in clinical outcomes of HF was successfully validated in the second independent population. Besides, the in vitro experiments revealed that G allele carriers were defective in β2AR-coupled inhibitory adenylate cyclase g (Gi) protein signaling.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
Similar articles
-
The genetics of cardiac failure: Role of a G protein-coupled receptor polymorphism in therapeutic response in an Indian population.J Clin Transl Res. 2021 Jul 30;7(4):501-510. eCollection 2021 Aug 26. J Clin Transl Res. 2021. PMID: 34541364 Free PMC article.
-
β-adrenergic receptor polymorphisms in susceptibility, response to treatment and prognosis in heart failure: implication of ethnicity.Mol Med Rep. 2013 Jan;7(1):259-65. doi: 10.3892/mmr.2012.1120. Epub 2012 Oct 9. Mol Med Rep. 2013. PMID: 23064657
-
Therapeutic Targets for Treatment of Heart Failure: Focus on GRKs and β-Arrestins Affecting βAR Signaling.Front Pharmacol. 2018 Nov 27;9:1336. doi: 10.3389/fphar.2018.01336. eCollection 2018. Front Pharmacol. 2018. PMID: 30538631 Free PMC article. Review.
-
Effect of ADRB2 polymorphisms on the efficacy of salmeterol and tiotropium in preventing COPD exacerbations: a prespecified substudy of the POET-COPD trial.Lancet Respir Med. 2014 Jan;2(1):44-53. doi: 10.1016/S2213-2600(13)70248-0. Epub 2013 Dec 5. Lancet Respir Med. 2014. PMID: 24461901 Clinical Trial.
-
Emerging concepts and therapeutic implications of beta-adrenergic receptor subtype signaling.Pharmacol Ther. 2005 Dec;108(3):257-68. doi: 10.1016/j.pharmthera.2005.04.006. Epub 2005 Jun 24. Pharmacol Ther. 2005. PMID: 15979723 Review.
Cited by
-
The genetics of cardiac failure: Role of a G protein-coupled receptor polymorphism in therapeutic response in an Indian population.J Clin Transl Res. 2021 Jul 30;7(4):501-510. eCollection 2021 Aug 26. J Clin Transl Res. 2021. PMID: 34541364 Free PMC article.
-
Vascular homeostasis at high-altitude: role of genetic variants and transcription factors.Pulm Circ. 2020 Nov 19;10(4):2045894020913475. doi: 10.1177/2045894020913475. eCollection 2020 Oct-Dec. Pulm Circ. 2020. PMID: 33282179 Free PMC article. Review.
-
Cardiovascular precision medicine - A pharmacogenomic perspective.Camb Prism Precis Med. 2023 Jun 29;1:e28. doi: 10.1017/pcm.2023.17. eCollection 2023. Camb Prism Precis Med. 2023. PMID: 38550953 Free PMC article. Review.
-
Pharmacogenetics to guide cardiovascular drug therapy.Nat Rev Cardiol. 2021 Sep;18(9):649-665. doi: 10.1038/s41569-021-00549-w. Epub 2021 May 5. Nat Rev Cardiol. 2021. PMID: 33953382 Free PMC article. Review.
-
Genetic polymorphisms are associated with individual susceptibility to dexmedetomidine.Front Genet. 2023 Aug 24;14:1187415. doi: 10.3389/fgene.2023.1187415. eCollection 2023. Front Genet. 2023. PMID: 37693312 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Research Materials
Miscellaneous
