

Addressing Clinical Inertia in Type 2 Diabetes Mellitus: A Review
- PMID: 30374807
- PMCID: PMC6223992
- DOI: 10.1007/s12325-018-0819-5
Addressing Clinical Inertia in Type 2 Diabetes Mellitus: A Review
Abstract
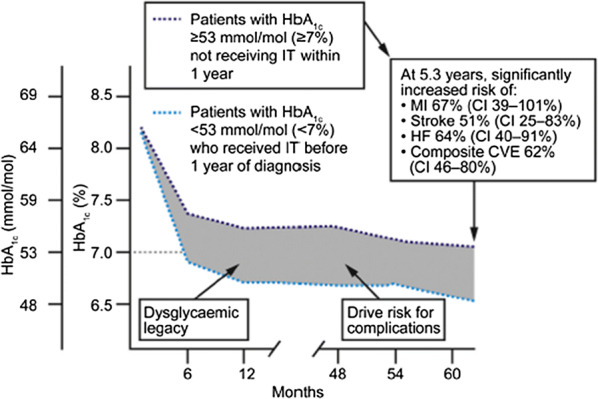
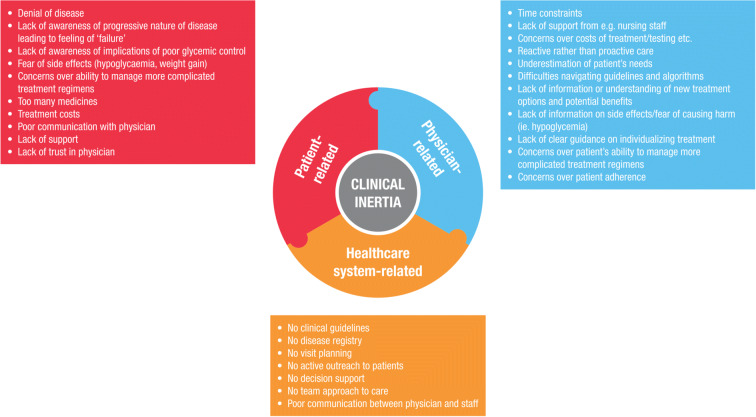
The current epidemic of type 2 diabetes (T2D) represents a significant global and national health concern. Globally, the prevalence of diabetes has doubled between 1980 and 2014. In 2014 the World Health Organization estimated that there were 422 million adults living with diabetes worldwide. In the USA, the number of people diagnosed with T2D is estimated to increase to over 70 million by 2050, putting an immense strain on the US healthcare system. Achieving glycemic control is widely acknowledged as the key goal of treatment in T2D and is critical for reducing the onset and progression of diabetes-related complications such as cardiovascular diseases, neuropathies, retinopathies, and nephropathies. Despite the increase in the availability of antihyperglycemic medications and evidence-based treatment guidelines, the proportion of people with T2D who fail to achieve glycemic goals continues to rise. One major contributor is a delay in treatment intensification despite suboptimal glycemic control, referred to as clinical or therapeutic inertia. Clinical inertia prolongs the duration of patients' hyperglycemia which subsequently puts them at increased risk of diabetes-associated complications and reduced life expectancy. Clinical inertia results from a complex interaction between patient, healthcare providers, and healthcare system barriers that need to be addressed together, rather than as separate entities. In this article we provide an overview of clinical inertia in the clinical management of T2D and provide suggestions for overcoming aspects that may have a negative impact on patient care.Funding: Sanofi US, Inc.
Keywords: Clinical inertia; Therapeutic inertia; Treatment intensification; Type 2 diabetes.
Conflict of interest statement
Jennifer Okemah has served on advisory boards for DexCom, and Sanofi; participated in speakers’ bureaus for DexCom, Insulet CPT, Medtronic CPT, Sanofi, and Sigma. John Peng has served on advisory boards for Sanofi. Manuel Quinones has served on advisory boards for AstraZeneca, Janssen Pharmaceuticals, Novo Nordisk, and Sanofi; participated in speakers’ bureaus for AstraZeneca, Janssen Pharmaceuticals, Novo Nordisk, and Sanofi.
Figures
Similar articles
-
Evaluation of the Clinical and Economic Burden of Poor Glycemic Control Associated with Therapeutic Inertia in Patients with Type 2 Diabetes in the United States.Adv Ther. 2020 Feb;37(2):869-882. doi: 10.1007/s12325-019-01199-8. Epub 2020 Jan 10. Adv Ther. 2020. PMID: 31925649 Free PMC article.
-
Factors Associated with Diabetes-Related Clinical Inertia in a Managed Care Population and Its Effect on Hemoglobin A1c Goal Attainment: A Claims-Based Analysis.J Manag Care Spec Pharm. 2019 Mar;25(3):304-313. doi: 10.18553/jmcp.2019.25.3.304. J Manag Care Spec Pharm. 2019. PMID: 30816810 Free PMC article.
-
Intensification of Diabetes Therapy and Time Until A1C Goal Attainment Among Patients With Newly Diagnosed Type 2 Diabetes Who Fail Metformin Monotherapy Within a Large Integrated Health System.Diabetes Care. 2016 Sep;39(9):1527-34. doi: 10.2337/dc16-0227. Epub 2016 Aug 12. Diabetes Care. 2016. PMID: 27519447
-
Approaches to rapid acting insulin intensification in patients with type 2 diabetes mellitus not achieving glycemic targets.Ann Med. 2018 Sep;50(6):453-460. doi: 10.1080/07853890.2018.1493216. Epub 2018 Aug 25. Ann Med. 2018. PMID: 30103624 Review.
-
Identification of barriers to insulin therapy and approaches to overcoming them.Diabetes Obes Metab. 2018 Mar;20(3):488-496. doi: 10.1111/dom.13132. Epub 2017 Nov 22. Diabetes Obes Metab. 2018. PMID: 29053215 Free PMC article. Review.
Cited by
-
Quality of Diabetes Care in the USA.Curr Cardiol Rep. 2021 Jun 3;23(7):73. doi: 10.1007/s11886-021-01503-5. Curr Cardiol Rep. 2021. PMID: 34081207 Review.
-
Addressing the Continuum of Dysglycaemia and Vascular Complications in Prediabetes and Type 2 Diabetes: Need for Early and Intensive Treatment.Diabetes Metab Syndr Obes. 2023 Jan 11;16:105-115. doi: 10.2147/DMSO.S396621. eCollection 2023. Diabetes Metab Syndr Obes. 2023. PMID: 36760588 Free PMC article. Review.
-
The public economic burden of suboptimal type 2 diabetes control upon taxpayers in Sweden: Looking beyond health costs.Diabetes Obes Metab. 2022 Jun;24(6):1038-1046. doi: 10.1111/dom.14667. Epub 2022 Mar 6. Diabetes Obes Metab. 2022. PMID: 35137507 Free PMC article.
-
Increasing the Adoption and Diffusion of a Novel Pharmacological Therapy That Is Both Mortality Reducing and Cost-Effective.J Am Heart Assoc. 2019 Feb 5;8(3):e011783. doi: 10.1161/JAHA.118.011783. J Am Heart Assoc. 2019. PMID: 30712487 Free PMC article.
-
Modern-Day Management of the Dysglycemic Continuum: An Expert Viewpoint from the Arabian Gulf.Diabetes Metab Syndr Obes. 2024 Dec 17;17:4791-4802. doi: 10.2147/DMSO.S491591. eCollection 2024. Diabetes Metab Syndr Obes. 2024. PMID: 39712240 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
