

Ruling out Appendicitis in Children: Can We Use Clinical Prediction Rules?
- PMID: 30374814
- PMCID: PMC6773677
- DOI: 10.1007/s11605-018-3997-1
Ruling out Appendicitis in Children: Can We Use Clinical Prediction Rules?
Abstract
Purpose: To identify available clinical prediction rules (CPRs) and investigate their ability to rule out appendicitis in children presenting with abdominal pain at the emergency department, and accordingly select CPRs that could be useful in a future prospective cohort study.
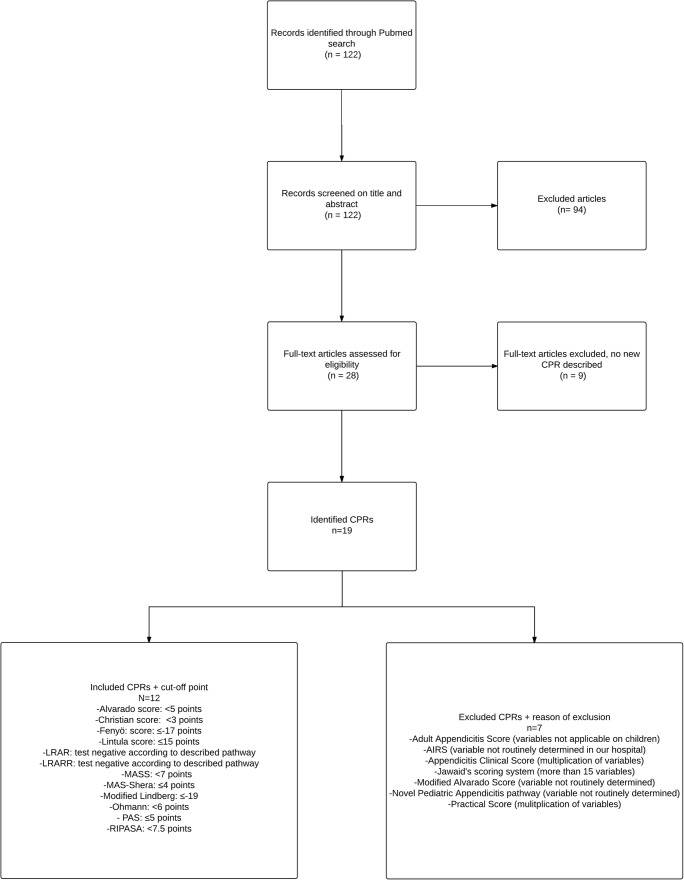
Methods: A literature search was conducted to identify available CPRs. These were subsequently tested in a historical cohort from a general teaching hospital, comprising all children (< 18 years) that visited the emergency department between 2012 and 2015 with abdominal pain. Data were extracted from the electronic patient files and scores of the identified CPRs were calculated for each patient. The negative likelihood ratios were only calculated for those CPRs that could be calculated for at least 50% of patients.
Results: Twelve CPRs were tested in a cohort of 291 patients, of whom 87 (29.9%) suffered from acute appendicitis. The Ohmann score, Alvarado score, modified Alvarado score, Pediatric Appendicitis score, Low-Risk Appendicitis Rule Refinement, Christian score, and Low Risk Appendicitis Rule had a negative likelihood ratio < 0.1. The Modified Alvarado Scoring System and Lintula score had a negative likelihood ratio > 0.1. Three CPRs were excluded because the score could not be calculated for at least 50% of patients.
Conclusion: This study identified seven CPRs that could be used in a prospective cohort study to compare their ability to rule out appendicitis in children and investigate if clinical monitoring and re-evaluation instead of performing additional investigations (i.e., ultrasound) is a safe treatment strategy in case there is low suspicion of appendicitis.
Keywords: Appendicitis; Children; Clinical prediction rules.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
References
-
- Warner BW, Kulick RM, Stoops MM, Mehta S, Stephan M, Kotagal UR. An evidenced-based clinical pathway for acute appendicitis decreases hospital duration and cost. J Pediatr Surg. 1998;33(9):1371–1375. - PubMed
-
- Boonstra PA, van Veen RN, Stockmann HB. Less negative appendectomies due to imaging in patients with suspected appendicitis. Surg Endosc. 2015;29(8):2365–2370. - PubMed
-
- Bakker OJ, PMNYH G, JBCM P, Kazemier G, Heij HA. Guideline on diagnosis and treatment of acute appendicitis: imaging prior to appendectomy is recommended. Ned Tijdschr Geneeskd. 2010;154:A303. - PubMed
-
- Van Rossem CC, Bolmers MDM, Schreinemacher MHF, Van Geloven AAW. Prospective nationwide outcome audit of surgery for suspected acute appendicitis. Br J Surg. 2016;103:144–151. - PubMed
-
- Blitman NM, Anwar M, Brady KB, Taragin BH, Freeman K. Value of focused appendicitis ultrasound and alvarado score in predicting appendicitis in children: Can we reduce the use of CT? Am J Roentgenol. 2015;204(6):W707–W712. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
